
Anatomy TUESDAY – Let’s Talk About Lats (Part 1)
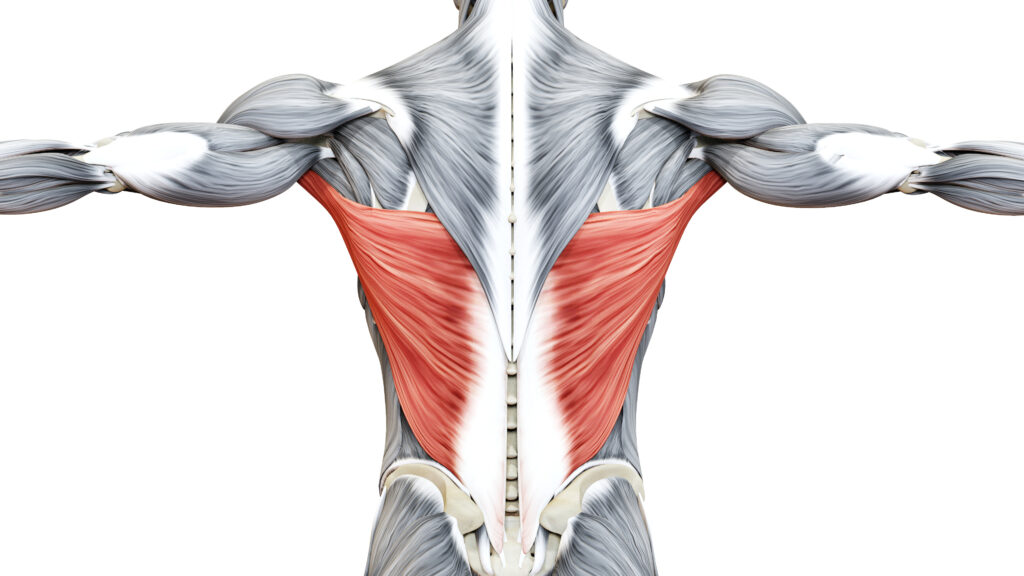
The latissimus dorsi is a powerful muscle often associated with pulling as it extends, adducts and internally rotates the shoulder. But my last two patients yesterday exhibited symptoms involving the lats that had nothing to do with the shoulder. The first was a person with chronic lower back pain and the second was someone with chronic neck pain. Let’s dive into the first case:
The patient is a 48-year old male who complains of severe chronic lower back pain that was exacerbated after a right total hip arthroplasty in June 2024. His pain is worse with sitting, which is required for his work, and will sometimes extend into the thoracic region. Here are some facts:
- R hip flexion is limited to 90/100 degrees (capsular endfeel)
- Weakness noted with MMT R hip flexion (painful in the hip), IR and ER
- Weakness noted with MMT trunk R rotation (painful in low back)
- Severe latissimus dorsi trigger points (lower thoracic spine and posterior axillary region) indicating over activity
- He ambulates with a supinated R lower extremity
The Lat/Glute Connection
A study of 61 right-handed males were divided into two groups: 31 with chronic lower back pain (LBP) and 30 healthy controls. The LBP group exhibited significant increase in latissimus dorsi activity and significant decrease in gluteus maximus activity as compared to the control group.
The attachment of the latissimus dorsi to the iliac crest, T7-L5 and lower ribs via the thoracolumbar fascia would indicate tightness of this muscle has the ability to create the following:
- lumbar extension (if tight biliaterally)
- anterior pelvic tilt (if tight bilaterally)
- anterior innominate rotation and opposite pelvic rotation (unilateral tightness) – over pronation scenario
- elevated iliac crest (unilateral tightness) – over supination scenario
In the case of this patient, it appears the #4 option is what is occurring.
Why does this matter? (Here’s what I’m going to do)
There appears to be a relationship to an overactive lat dorsi and weak gluteus maximus. A complete treatment plan includes activating the gluteus maximus AND releasing the latissimus dorsi. Trying to regain more hip flexion ROM will assist in decreasing lumbar flexion forces while sitting. But if we are not able to increase hip flexion range, EMG studies show greatest activation of the gluteus maximus at 0 degrees of extension. In other words, employing isometric activation of the glutes prior to squatting/lunging may also assist inhibiting the latissimus dorsi.
It is important to check and consider latissimus dorsi contribution to lower back pain and gluteal inhibition. The lats don’t just work the arms. That’s food for thought.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








