
Anatomy TUESDAY – Clinical Anatomy Pearls 3 – Achilles Tendon
Tendinopathy is one of the most common conditions encountered in musculoskeletal practice. Whether treating runners with Achilles pain, overhead athletes with rotator cuff symptoms, or office workers with lateral elbow pain, clinicians routinely assess and manage tendon-related disorders.
Yet a common misconception persists:
A tendon is a tendon is a tendon.
In reality, tendons differ significantly in their anatomy, vascularity, loading characteristics, and healing potential. These differences help explain why some tendons respond rapidly to rehabilitation while others remain stubbornly symptomatic for months.
Let’s take a look at four commonly injured tendons and their characteristics, starting with the Achilles Tendon.
ACHILLES TENDON
The Achilles tendon is often considered the ultimate energy-storing tendon. During running and jumping, it functions like a spring, storing mechanical energy during loading and releasing it during propulsion. This allows for remarkable efficiency in human movement.
However, this role comes at a cost.
The Achilles experiences some of the highest loads in the human body—often exceeding six to eight times body weight during running.
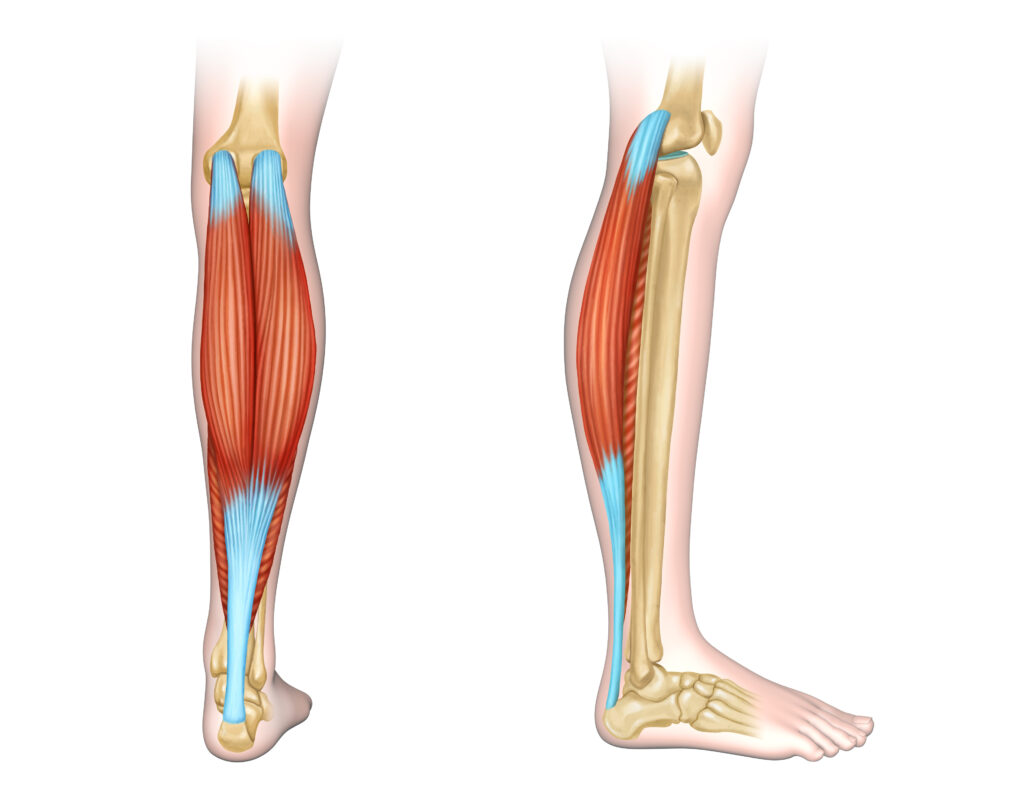
The Achilles tendon does not have a true synovial sheath. Rather, it is surrounded by a paratenon, composed of a single layer of cells and a membrane of loose areolar tissue. The paratenon is connected to the muscular fascia proximally and the periosteum of the calcaneus distally. It functions to allow the tendon to glide 1.5 cm cephalocaudally during plantarflexion and dorsiflexion.
The blood supply to the Achilles tendon is housed in the paratenon with branches of the the posterior tibial artery supplying the superior, inferior and medial portions of the tendon. The mid-portion of the tendon is thinner and relatively hypovascular being supplied by the branches of the peroneal artery located on the lateral side. Due to small cross-sectional size and decreased blood supply, an area of the Achilles tendon 3-5 cm proximal to the calcaneal insertion is commonly associated with mid-portion Achilles tendinopathy.
Clinical implications:
- Mid portion Achilles tendinopathy is most common and associated with over pronation of the limb. Lack of ankle dorsiflexion and a weak gluteus medius are often associated with over pronation. Fix these first prior to progressively loading the tendon.
- Insertional tendinopathy is often associated with over supination of the limb. Lack of subtalar joint eversion or a leg that feels too short may contribute to over supination. Key trigger points that “shorten a leg”: quadratus lumborum and psoas major
- Ultrasound to mid portion of tendon may help increase blood flow and enhance healing
- Parallel friction massage with the tendon on a slight stretch may help restore gliding of the paratenon
- Graded and progressive loading is key in strengthening the Achilles tendon. Tendon strength has been shown to increase with speed. For instance, when runners hit 180 strides per minute (each foot hitting the ground 90 times), physiological stiffening occurs. This is a good thing and prevents injury.
Why does this matter?
The Achilles tendon is unique in its make-up and function in that it is designed to dissipate forces exceeding 6-8x your body weight during walking, running and jumping. Understanding tendon anatomy allows clinicians to make better decisions regarding diagnosis, prognosis, load management, and patient education.
Join me next week when we dive a bit deeper into the the supraspinatus tendon, the most commonly injured rotator cuff tendon.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








