
Kinesiology THURSDAY – Matthew Stafford’s Aggravated Disc

At 38 years old, Matthew Stafford is no spring chicken but still a force in the NFL. In August 2025, he suffered an aggravated disc in his back at training camp that was treated with an epidural injection. His history of back injuries has some holding their breath as the NFL season gets underway:

- 2019 – multiple small fractures in his back ended his then-record consecutive winning streak
- 2021 – mild lumbar sprain
- 2024 – lumbar sprain/pull
- 2025 – mild disc bulge
He also has a history of multiple right ankle sprains (2020 and December 2024).
Stafford is also known for his no-look pass, a move that requires him to square his pelvis and shoulders up in one direction and throw in the opposite:
Herniated discs are often aggravated with excessive lumbar rotation. With the facet joint orientation largely in the sagittal plane, the lumbar spine is not designed to rotate.
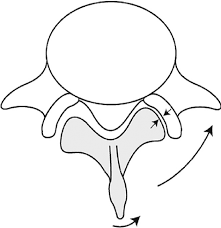
Approximately 10˚ of rotation is supposed to occur in the lumbar spine with almost half of that occurring at L5/S1, making the lower lumbar segments most susceptible to rotational injury. (The facet joint orientation starts to change at this level).
A successful epidural steroid injection simply confirms the presence of nerve root inflammation. It addresses the “what?” but not the “why?” behind the herniation.
Functional rotation of the body is designed to occur at three key areas: subtalar joint (ankles), hips and thoracic spine. The better you rotate here, the less your lumbar spine has to rotate.
What Would I Do?
If I was charged with keeping Matthew Stafford’s back healthy, here is what I would do:
- Check his right ankle for normal dorsiflexion and eversion. Lack of motion in these directions will prevent his right gluteus maximus, the one that powers his throw, from activating normally. The stronger his right glute max, the less rotational force is transferred to his lumbar spine
- Check for adequate hip rotation. Does he have a normal FABER and piriformis test? Can his hip open up and close down (ER and IR respectively) without a pinch or a jam? Some culprits to limited hip rotation: piriformis, posterior gluteus medius, psoas major, vastus lateralis, lateral gastrocnemius.
- Check pelvic alignment as it can affect hip rotation
- Assess thoracic rotation and perform the thoracic sequence to normalize. This is especially important with his no-look pass that requires him to rotate primarily above the hips during the throw
Why does this matter?
Herniated lumbar discs don’t occur in isolation, usually occurring with repetitive flexion and rotation occurring in the lower lumbar segments. Herniated discs may retract over time, but only if rotational forces are mitigated. There are two ways to look at this:
- Stabilize the lumbar segments (this is like putting a bandaid on a gusher). With multiple times your body weight in ground reaction forces barreling towards the lumbar spine, this method is
- Get the rotation to happen where it is designed to happen. Make the path of least resistance the path through the ankle, hips and thoracic spine so that by the time the rotation hits the lumbar spine, it is a whimper.
I choose #2 all day long, whether I’m treating Stafford or not. Take your ears and listen to the pain. Then take your eyes and look somewhere else for the solution.
Wishing Stafford a successful season. (Until the Rams play the Lions).
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








