Kinesiology THURSDAY – A Case of Post-Surgical Right Knee Plica Syndrome
One of my favorite things is to hear from a former student or seminar participant regarding a patient case. Often our exchanges are short, but I wanted to illustrate how much information can be yielded by figuring out the answers to a few key questions. Here is one I got yesterday:
I have a patient who had microfracture surgery on his (right) knee in May. He still is unable to do eccentric, quad, lowering bodyweight downstairs without excruciating pain. He is having quad tendon debilitating pain at this point. We’ve tried dry needling we’ve done cupping to the quad we’ve cut out quad exercises completely. We’ve done only eccentric exercises, I feel like we’ve tried it all. Any suggestions??
She added these details from his chart: Right knee scope with resection of plica and chondroplasty with microfracture of trochlear chondral defect. She also reported that he lacked terminal knee extension.
Let’s break this one down…
- Microfracture surgery involves drilling small holes into the bone to promote growth of articular cartilage. It is often performed on athletes who have sustained joint injuries.
- Surgery was performed over 5 months ago. His heightened pain response is unusual for this late post-surgically. Bone usually heals in 6-8 weeks
- The trochlear groove is the area between the femoral condyles that articulates with the patella
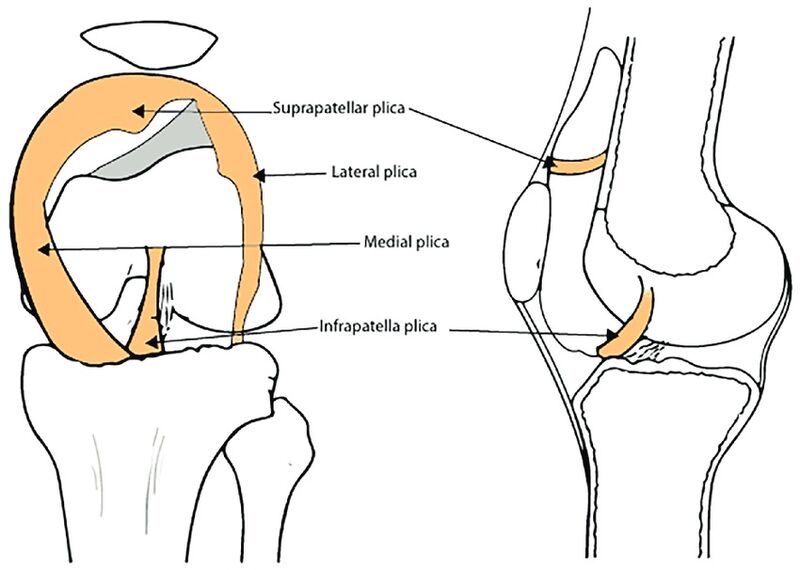
- The plica (as illustrated in the picture above) is an extension of the synovium. Though the plica has several parts, the medial plica is the symptomatic area, with potential of becoming impinged if the patella rides too medially. The medial plica also sends an extension to the area of the patellar tendon.
- The only time the patella is not in contact with the trochlea is in terminal knee extension. A knee that does not fully extend has constant patellofemoral pressure
This was my response:
“Check for trigger points in the gastrocs and hamstrings. A medial gastroc trigger point is common and will perpetuate over supination which drives that force right up to the knee. So, today work on releasing the gastrocnemius, the popliteus, the medial hamstring and tibialis anterior and posterior. Check all those things and fix what you find. And then have him retry movements that were formally painful. Let me know what happens.
Also make sure he can hyperextend the knee even passively. If his knee is always slightly bent, the patella and trochlea will take on constant pressure.”
I asked for a post-treatment report. She replied, “He said ‘I feel better’ but pain wasn’t gone”. When asked which of the mentioned muscles had the worst trigger points, she replied: Medial gastroc and lateral hamstring. Medial gastroc was the worst.
What Would I Do?
- Check the subtalar joint for eversion. A lack of eversion increases medial knee joint line compression and tibial internal rotation which results in excessive medial patellofemoral compression
- Release the medial gastroc and lateral hamstring trigger points
- Stretch the knee into terminal knee extension. If the patient feels a pinch in the front instead of a stretch in the back, releasing popliteus and medial gastroc trigger points will help. Also, when you stretch place an external rotation force on the tibia. Remember, in terminal knee extension, the tibia must externally rotate.
- Retrain ankle dorsiflexion and eversion: gravity drop, BOSU rockers, heel-toe line walking, balance on Airex pad, medial reach with leg (once tolerated)
- Lengthen lateral hamstring: revolving triangle, anterior cone touch with opposite hand, anterior/lateral pulley low row
- Train terminal knee extension: standing TKE with tubing, long stride walking
Notice how none of these things say strengthen the quad. Eventually, I would. But if the quad is weak because of pain, doing quad exercises in the sagittal plane is not the right move at this time. Fixing lower leg mechanics in the transverse plane to alleviate pressure on the medial knee and patellofemoral joint is key.
When a post-surgical knee isn’t responding as expected, it’s best to keep your ears on the part crying out in pain and take your eyeballs and look elsewhere for the source of the problem. And be curious. Have an expectation of what your treatment outcome should be and if you aren’t getting the result you want, look for another path. I am confident he is in great hands.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]