
Anatomy TUESDAY – The Hidden Nerves Behind Joint Pain
“My doc told me I was bone-on-bone and that’s why my knee hurts,” my patient said.
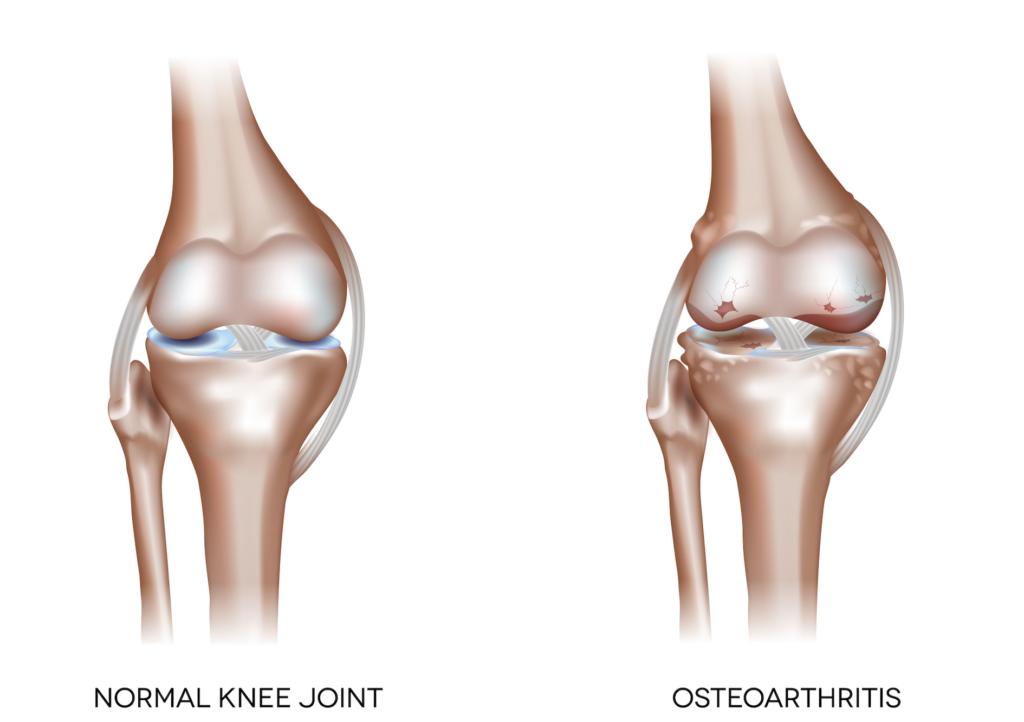
The wearing away of joint cartilage is often used as an explanation for knee pain. But cartilage doesn’t contain nerves. If cartilage can’t send pain signals, then what is really causing the pain?
The answer lies in the hidden nerves inside the joint—and the tissues that surround the cartilage. While cartilage itself is aneural (without nerves), many other joint structures are densely innervated. These include: synovium, the joint capsule, ligaments, subchondral bone (the bone beneath the cartilage) and the lining of the bone.
These tissues contain specialized sensory nerve endings called nociceptors—pain receptors designed to detect potential threat or tissue stress. When these nociceptors are activated, they send signals through peripheral nerves to the spinal cord and brain, where pain is perceived. So while cartilage damage may be part of arthritis, the pain usually originates from these surrounding, innervated tissues.
Meet the Pain Fibers: A-Delta and C Fibers
Two main types of nerve fibers transmit joint pain:
A-delta fibers: Fast-conducting fibers responsible for sharp, localized pain.
C fibers: Slower fibers that produce dull, aching, or throbbing pain.
In many chronic joint conditions, especially osteoarthritis, C fiber activity becomes more prominent. This explains why joint pain often feels deep, diffuse, and persistent rather than sharp and precise.
When the joint becomes irritated, the body releases inflammatory chemicals (prostaglandins, bradykinin, etc). These chemicals doin’t just signal damage, they sensitize nociceptors in a process called peripheral sensitization, making nerves more reactive.
This means:
- Swelling increases pain
- Even light pressure may feel exaggerated
- Movements that were once tolerated become uncomfortable
If nociceptors are activated for a prolonged period, changes can occur not just in the joint but in the nervous system itself. The nervous system becomes more efficient at producing pain signals, a phenomena known as central sensitization. This may show up as:
- Pain disproportionate to imaging findings
- Widespread sensitivity (“I hurt all over”)
- Pain that lingers after activity
Why does this matter?
Cartilage may be the most visible structure in joint disease, but it is not the primary source of pain. This is great news. If the real drivers of pain are the hidden nerves embedded in synovium, capsule, ligaments and bone, then the conversation shifts away from “wear and tear” (who’s only solution is a joint replacement) and toward a more accurate view of joint pain being a dynamic interaction between tissue health and nervous system sensitivity.
Managing swelling and correcting joint mechanics with biomechanical approach yields many treatment options. It allows a clinician to provide an individualized solution to joint pain and raise the threshold of the A and C pain receptors.
I often tell patients they know they are getting better not because they never have pain, but because their recovery from an irritation is quicker. It gives patients hope and clinicians work to do. We can’t restore joint cartilage, but we can do a lot about normalizing joint mechanics to minimize irritation of the bone, joint capsule and ligaments. Consider the source and treat it.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








