
Kinesiology THURSDAY – Biomechanics of Anterior Shoulder Instability

Among overhead athletes presenting to sports medicine clinics with shoulder pain, anterior instability or microinstability is believed to contribute to approximately 15–25% of cases, although it is frequently associated with other disorders rather than occurring in isolation, such as: scapular dyskinesis, internal impingement, SLAP lesions, partial articular-sided rotator cuff tears and glenohumeral internal rotation deficit (GIRD).
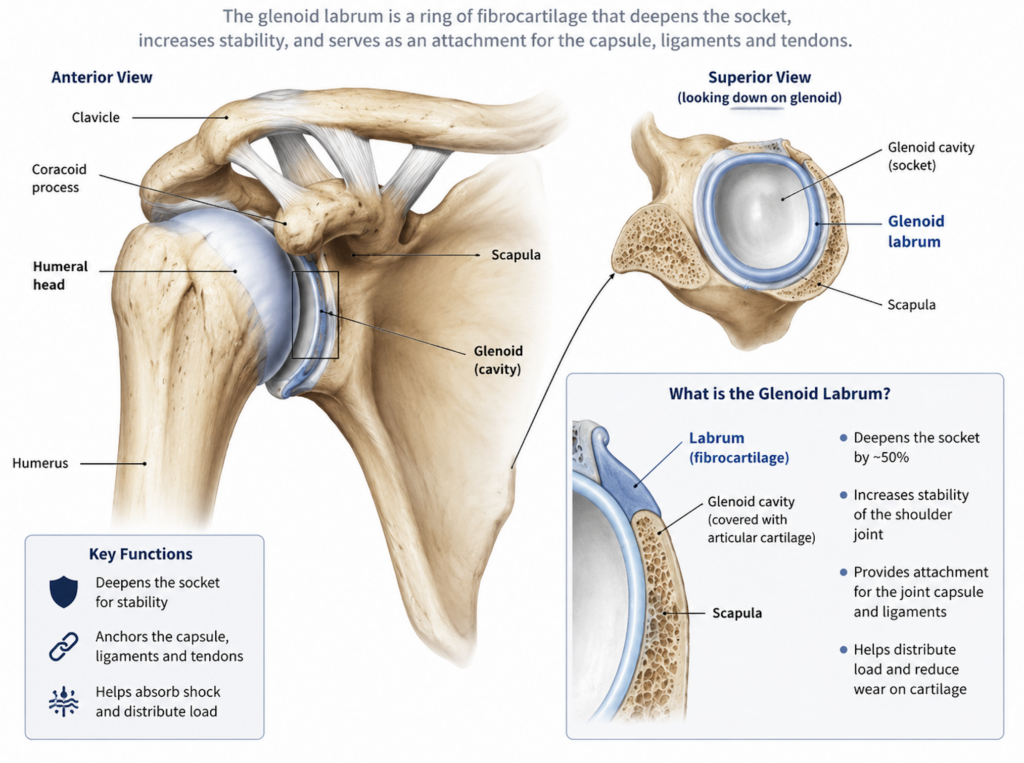
The glenohumeral joint is one of the most mobile joints in the body, with the humeral head being 1.5-2x the diameter of the glenoid fossa. The glenoid labrum deepens the socket, adding 50% more stability, but the stability of the joint is dependent on way more than a fibrocartilaginous ring.
Anterior migration of the humeral head occurs with external rotation of the shoulder. But during function, the ground reaction forces traverse many joints prior to impacting the glenohumeral joint. During batting and pitching, angluar velocity of the shoulder ranges from 1000˚/sec to 6500˚-7500˚/sec respectively. Bat speed can reach up to 80 mph. Take a look at this picture:

This is a left handed batter who has already swung at the ball. The batter’s right shoulder is in a position of end range external rotation, but force dissipation occurs starting from the ground up. In order to successfully dissipate forces associated with the swing, the following must occur:
- Subtalar joint eversion (his right foot is already inverted as he is at the end of his swing) – eversion internally rotates the tibia, loading the lateral hamstring (bicep femoris)
- Right knee flexion – loads the quadriceps
- Right hip flexion/internal rotation – loads the gluteus maximus
- Right thoracic rotation and left thoracic side bending – loads the right external oblique and left internal oblique
- Right scapular retraction – loads the serratus anterior and pec minor and THEN
- Right glenohumeral external rotation – which loads the internal rotators of the shoulder (pec major, subscapularis, teres major, latissimus dorsi)
In the cases of glenohumeral anterior instability, strengthening the shoulder muscles barely scratches the surface. Too much motion happening in one place usually signals a lack of motion somewhere else. Hypomobility in one joint breeds hypermobility in another. What is often viewed as weakness of shoulder internal rotators causing instability is more often overload of the shoulder stabilizers due to lack of force dissipation distally in the biomechanical chain.
Why does this matter?
Successful treatment of joint hypermobility requires more than just strengthening the stabilizers of the shoulder, especially when protecting against high velocity activities. This is like putting a bandaid on a gusher.
Assessing related joints along the biomechanical chain from the ground up and fixing what you find will often yield more successful outcomes. Force follows the path of least resistance. In hypermobility, we need to make the right path the path of least resistance.
So, use your ears to listen to the joint in pain and then take your eyeballs and look elsewhere.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








