Kinesiology THURSDAY – L5 Anger Management
This is a blog about thinking outside of the box, so today, I thought I’d talk about one of the most common pathologies I treat, sciatica, and a cause that is often overlooked. Sciatica simply describes an impingement of the sciatic nerve that causes referred pain usually into the buttock and posterior thigh to the level of the knee. The sciatic nerve is a large nerve derived from L4-S3, but the most often insulted level is L5-S1.
Why is that?!
The five segments of the lumbar spine have a facet joint orientation that is largely in the sagittal plane, meaning they are designed to allow liberal amounts of flexion/extension, but limit rotation. In fact, each level allows only 1-2 degrees of rotation, for a total of 10 degrees of rotation over the five segments. L5 facet joint orientation is different from the segments above, angling slightly more towards the frontal plane as it articulates with the sacrum, allowing for 4 degrees of rotation.
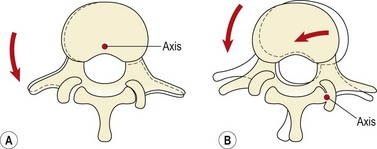
If you look at the picture above, you can see that rotation to the left closes the facet joint (and foramen) on the right side, potentially impinging the nerve.
Let’s take a look at a functional rotational pattern:

This lateral low row is an example of a pattern that is used everyday when someone lifts. Clearly, there is way more than 4 degrees of rotation (closer to 90 degrees) and it is made possible by the biomechanical chain including:
- 6-8 degrees of right subtalar joint eversion
- 30-40 degrees of knee flexion (which loads the quad)
- 40-45 degrees of hip flexion/internal rotation (which loads the glute and hamstrings) THEN
- 10 degrees of lumbar spine rotation to the right (which closes off the left facet)
If steps 1-3 are limited, then L5 takes a big hit. More than 5 degrees of rotation will occur, causing L5 nerve root impingement and irritation. A pinched nerve will swell and swelling compromises the foraminal space causing further or chronic impingement. An angry L5.
Why does this matter?
Often, we diagnose sciatica and have a “protocol” in our heads. it may include traction, modalities to the involved side and some stretches to the piriformis. But if you understand the scenario described above, you would realize that more times than not, the cause of sciatica is tightness on the OPPOSITE leg. Assess for trigger points in the opposite:
- medial gastrocnemius (limits eversion)
- lateral hamstring (limits tibial IR)
- vastus lateralis, adductor, posterior gluteus medius and piriformis (limits hip IR)
Fix what you find, even if it’s not on the side of pain. Especially if its not on the side of pain. That’s thinking outside of the box.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]