
Kinesiology THURSDAY – Six Degrees to a Stuck Subtalar Joint
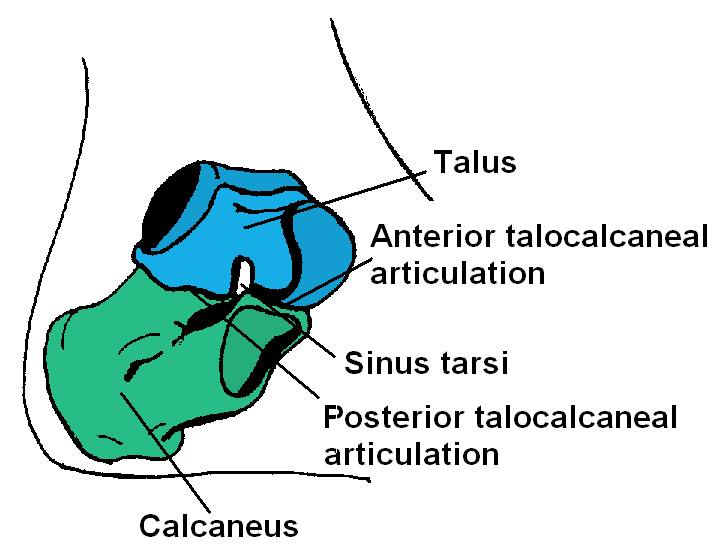
The subtalar joint (STJ), the articulation between the talus and the calcaneus, is largely designed to allow for pronation (eversion) and supination (inversion) of the ankle. The foot is the first point of contact on the ground, and the first of many points to absorb the shock of ground reaction forces when we walk, run or jump. Subtalar joint eversion lies at the heart of this shock absorption. Lack of eversion, or a “stuck” subtalar joint, is often the cause of over supination injuries, such as recurrent lateral ankle sprains, adductor strains (groin pulls), ITB friction syndrome and sacroiliac (SI) joint dysfunction. Let’s look at six degrees to a stuck subtalar joint:
- Previous lower extremity injury/surgery – Total knee/hip replacement, arthroscopic surgeries to the knee, ankle sprains, ligament tears of the knee or even chronic lower back pain cause a protective response of the lower extremity that includes supination of the subtalar joint. If the subtalar joint stays supinated, then the muscles of the lower extremity are not taxed (eccentrically loaded) as heavily. Unfortunately, long after the surgery or injury, this lack of STJ eversion can remain, altering lower extremity function. The FIX: restore STJ eversion with this functional mobilization.
- A leg that feels too short – The STJ will remain inverted to compensate for a functionally shorter leg. Trigger points in the quadratus lumborum and psoas major may cause a leg to feel shorter. A posteriorly rotated innominate will also cause a leg to function shorter. The FIX: Correct pelvic alignment and evaluate and treat trigger points in the quadratus lumborum and psoas major.
- Trigger points in the posterior tibialis and flexor hallucis longus – These trigger points are palpated along the medial aspect of the tibia. Tightness of these muscles cause inversion of the ankle as they pass posterior to the medial malleolus. The FIX: Release trigger points by performing deep tissue mobilization along the medial tibia.
- Trigger points in the anterior tibialis – These trigger points are palpated on the lateral side of the tibia and also cause inversion as the muscle attaches to the base of the first ray of the foot (metatarsal and cuneiform). The FIX: Release fascia and trigger points with these techniques.
- Trigger points in the medial gastrocnemius – This trigger point is most common following a surgical procedure. This muscle attaches at the calcaneus causing inversion of the foot. The FIX: Deep tissue massage to the medial gastrocnemius followed by stretching using downward dog or the gravity drop
- A big toe that won’t extend (decreased 1st MTP extension) – You should be able to passively extend your big toe 45-65 degrees. Lack of this flexibility will cause compensatory supination of the foot. The FIX: Stretch your big toe back into extension or perform a posterior glide of the proximal phalanx on the metatarsal head to promote extension. Then try walking on your toes to improve extension range of motion.
Why does this matter?
Lack of subtalar joint eversion will inhibit activation of key muscles up the biomechanical chain: gluteus maximus, gluteus medius and quadriceps. A stuck subtalar joint may also alter leg length. In cases of chronic pain or a history of lower extremity surgery or injury, check the subtalar joint and restore eversion.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








