
Kinesiology THURSDAY – Tobias Myer’s Left Internal Oblique

Years ago, I wrote an article about the prevalence of internal oblique tears in MLB players. The injury usually occurs opposite to the side of the throwing arm in pitchers and may occur on either side in other players. I did a deep dive into what might be causing the internal oblique tears/strains, which were confirmed by MRI. That was in 2008. I just did a quick search of internal oblique tears sidelining MLB in 2025 more than 10 are listed. Tobias Myers, pitcher for Milwaukee Brewers, is one of them. And this isn’t his first internal oblique injury.
What does the internal oblique do?
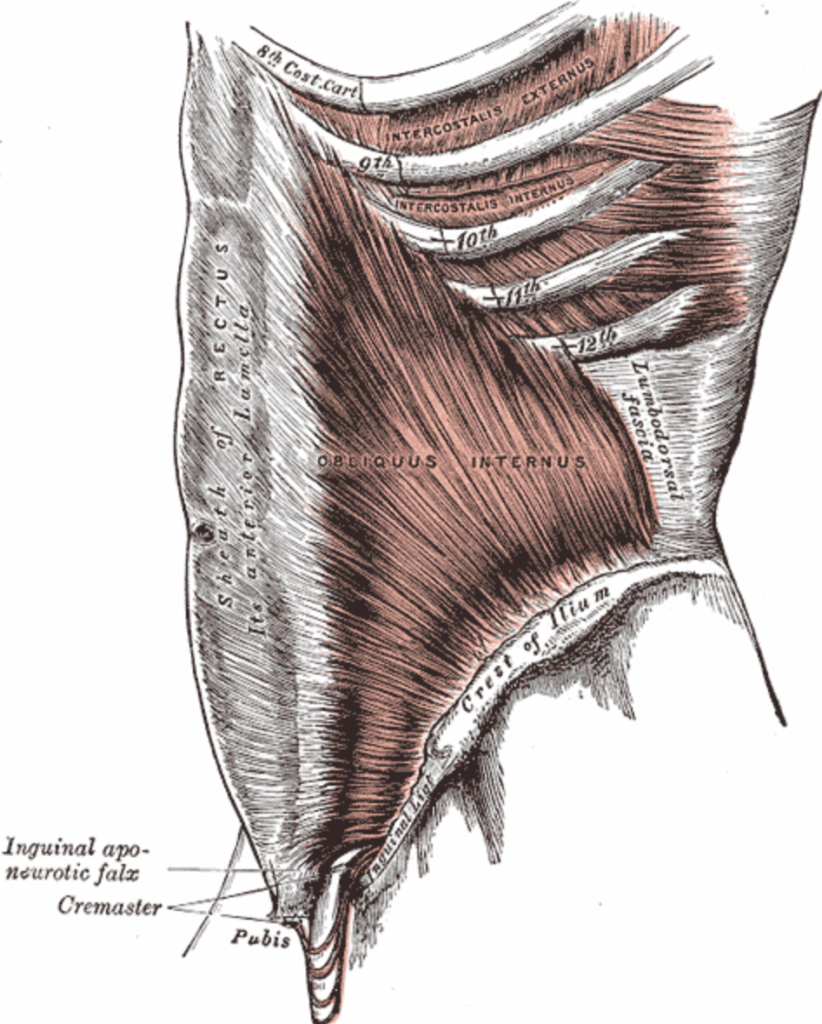
The internal oblique originates from the lumbar fascia, iliac crest and inguinal ligament and inserts on the 8th-12th ribs, pubic crest and aponeurosis of the rectus muscle. Functionally, it works in conjunction with the opposite external oblique and gluteus maximus (dominant side) to decelerate the cocking phase of a throw and to accelerate the throw. In other words, the opposite gluteus maximus and internal oblique are functionally synergistic. The gluteus maximus is the larger and more powerful of the two muscles. Inhibition or weakness of this muscle will automatically require more force to be dissipated and generated by the opposite internal oblique, thereby predisposing it to injury.
The internal oblique is placed in a long/weak (inhibited) position in the following ways:
• Sagittal plane – anterior pelvic tilt
• Frontal plane – pelvic drop (weak opposite gluteus medius)
• Transverse plane – ipsilateral pelvic rotation
Internal studies at MIHP reveal most right handed individuals have a predisposition to a pelvis that is rotated to the left. This pelvic rotation not only places the left internal oblique in a long weakened position, but it also places the right hip in relative external rotation (a position that is inhibitory to the gluteus maximus).
How can we help Tobias?
A clinician can check this by assessing the athlete’s pelvis in supine. Does the left ASIS appear closer to the table? Next, assess the isometric strength of the gluteus maximus via isometric prone hip extension with the hip slightly abducted and externally rotated. Is the right one weaker? Is the right foot more externally rotated in standing? If the answer to these two questions is yes, then you just may have solved the puzzle to the chronically injured internal oblique.
The most efficient fix requires manual correction of pelvic malalignment. Innominate rotations, sacral torsions and lumbar somatic dysfunction are often found and, if corrected, will immediately correct the pelvic rotation.
Next, therapeutic exercises must target strengthening of the gluteus maximus on the dominant side, the one opposite to the injured internal oblique. Core training that focuses solely on trunk rotation and not allowing hip rotation may be an aggravating factor.
A targeted hip strengthening program should produce positive results in just a few sessions.
Why does this matter?
Internal oblique tears/strains are sidelining MLB players across the country. But it’s not just them. I sent my 2008 article to all the MLB teams listing players with this injury (including the Detroit Tigers who had three side lined players with this injury at the time) and received no response. So I put it out on the internet somewhere and guess who I heard from? Cricket players in India and a serious recreational table tennis player who tore his left internal oblique during a match. The latter had just completed rehabilitation of a right total hip replacement.
I have never met Tobias or seen a Milwaukee Brewer’s game but maybe let’s help Tobias and other MLB players get back on the field. Or maybe you can share this with some cricket and table tennis players who could use our help.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








