Muscle Minute TUESDAY – Meet the Lateral Gastrocnemius

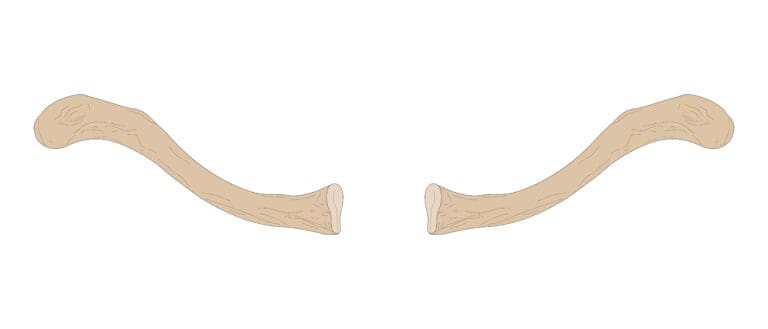
It’s easy to think of the gastrocnemius as a unified muscle, but nothing could be further from the truth. The lateral gastrocnemius (LG) is different in make-up and function than it’s counterpart, the medial gastrocnemius (MG) and may explain why the MG is more often injured than the LG. Let’s take a deeper dive.
| Origin | lateral surface of lateral femoral condyle |
| Insertion | calcaneus via Achilles tendon |
| Action | plantarflexion, knee flexion, femoral external rotation |
| Innervation | tibial n. (S1, S2) |
| Antagonists | tibialis anterior, medial gastrocnemius |
The Real World Lateral Gastrocnemius
- LG has a longer fiber length than the MG, giving it greater velocity potential than MG, which means it can generate greater force and is less prone to injury. (Shorter muscle fibers are more prone to injury during eccentric exercise)
- LG has a bipennate structure, where as the MG as a unipennate structure. Bipennate muscles tend to display greater stiffness.
- LG shows less fatigue than MG after maximal volitional contraction
- Cross-sectional area of LG is smaller than MG
- Compared to the MG, the LG motor unit activity was silent during standing.
- During heel raises, the LG was seen to be more active with toe-in position v. toe-out position (where MG was more active)
An unmentioned task…
It was interesting to note that all the references I checked out talked about the medial gastrocnemius being more prone to injury and fatigue than the lateral during ankle plantarflexion activities. Nothing mentioned the potential action that occurs at the femur, namely the deceleration of femoral internal rotation, which makes LG a functional synergist to the gluteus maximus. Trigger points in LG (which are common) signal a femur that is chronically externally rotated. And in regards to transverse plane movement at the knee, the LG and MG are functionally antagonistic, which means if one is tight, the other becomes long/weak and prone to injury.
Here’s a short list of why this matters:
- If the MG is injured, there may be a trigger point in the LG
- If LG has a trigger point, this may mean the femur is externally rotated making it difficult to recruit gluteus maximus (butt will be shut off)
- LG may be shortened (or inhibited) with a toe-out position common in over pronators and more activated with a toe-in position common in over supinators
Conventional thinking says: The medial and lateral gastrocnemius plantarflex the ankle and flex the knee
Real World Thinking says: The two parts of the gastrocnemius are very different and their make-up, function and fatigueability may explain why the MG is more often injured than the LG. LG trigger points should be considered when treating MG injury and overuse injuries that involve chronic femoral external rotation (i.e. medial patellofemoral pain, medial meniscus impingement, piriformis syndrome).
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]