Anatomy TUESDAY – Clinical Anatomy Pearls 1 – Pain Referral Patterns

A patient points to the outside of their shoulder and says, “My shoulder hurts.” Another rubs the front of their knee and complains of persistent pain with stairs. A third describes aching in their hip that radiates into the thigh. While it may seem intuitive to focus on the area where the patient experiences pain, experienced musculoskeletal clinicians know an important truth:
The source of pain is not always the source of symptoms.
Understanding regional anatomy and referral patterns is one of the most valuable skills clinicians can develop. Without it, treatment may be directed at the wrong tissue, the wrong region, or even the wrong diagnosis.
Patients naturally associate pain with the structure directly beneath it. Unfortunately, the nervous system doesn’t always follow the same logic. Numerous anatomical structures can refer pain to distant locations, including: joints, muscles, tendons, ligaments, nerves and intervertebral discs.
As a result, the location of symptoms may provide an important clue, but it should never be the sole determinant of diagnosis. The clinician’s role is to identify not just where pain is felt, but where it originates.
Let’s take a look at three common examples.
The shoulder pain that isn’t…
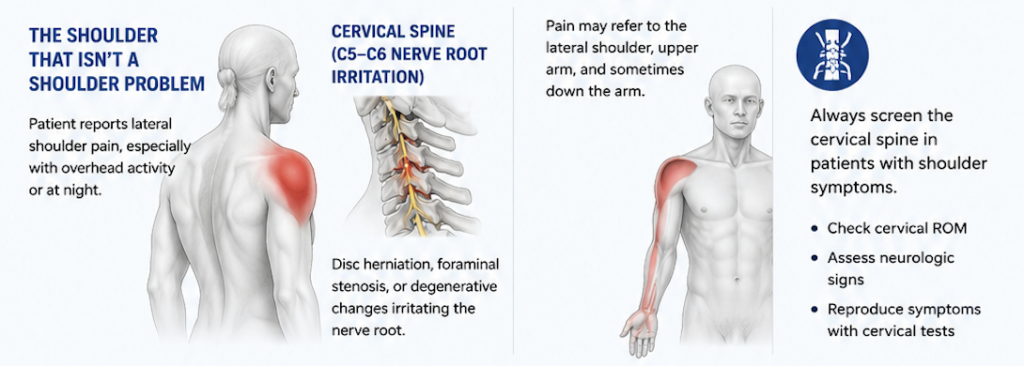
Lateral shoulder pain is one of the most commonly reported upper extremity symptoms that is often attributed to a deltoid injury. Adhesive capsulitis, rotator cuff tears and subacromial bursitis often refer pain into the lateral shoulder and the following may also cause lateral shoulder pain:
- C5-C6 nerve root irritation – pain in the lateral shoulder elicited with cervical compression testing
- Infraspinatus trigger points – most common trigger point located at inferior angle
- Supraspinatus trigger points – in muscle belly above spine of the scapula
- Upper trapezius tightness causing cervical compression – in muscle belly lateral to base of the neck
Here’s a video that will help you palpate key muscles of the shoulder.
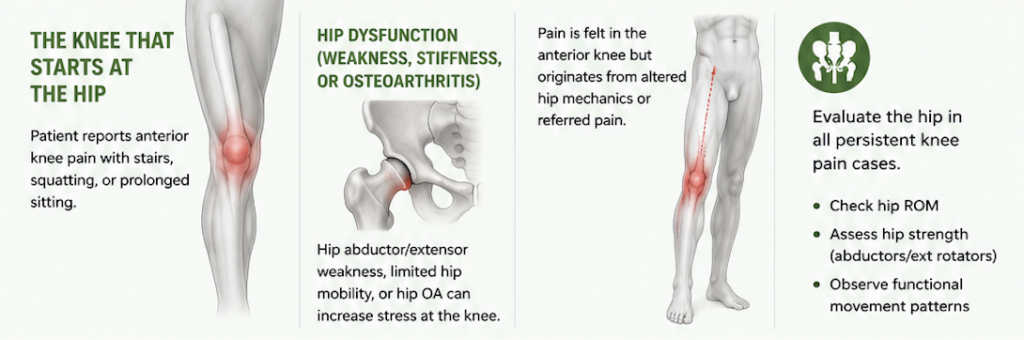
The knee pain that isn’t…
Knee pain is another area where clinicians can be misled.
Patients frequently present with anterior knee pain, particularly during squatting, stair climbing, or prolonged sitting. While local knee structures deserve attention, deficits at the hip often contribute significantly. Here is a short list of things that refer pain to the knee:
- L3 nerve root compression – not as common as compression in some of the lower levels, but associated with trigger points in psoas major and quadratus lumborum
- Rectus femoris trigger point – refers pain to anterior knee
- Adductor magnus trigger point – refers pain to medial knee
- Osteoarthritis of the hip – knee pain referred usually in end ranges of hip flexion and internal rotation
- Over pronation of the limb – weak gluteus medius and gluteus maximus
- Over supination of the limb – lack of subtalar joint eversion
Treating the knee without evaluating the hip, ankle and lumbar spine may result in incomplete improvement and unnecessary frustration for both clinician and patient.
The hip pain that isn’t…
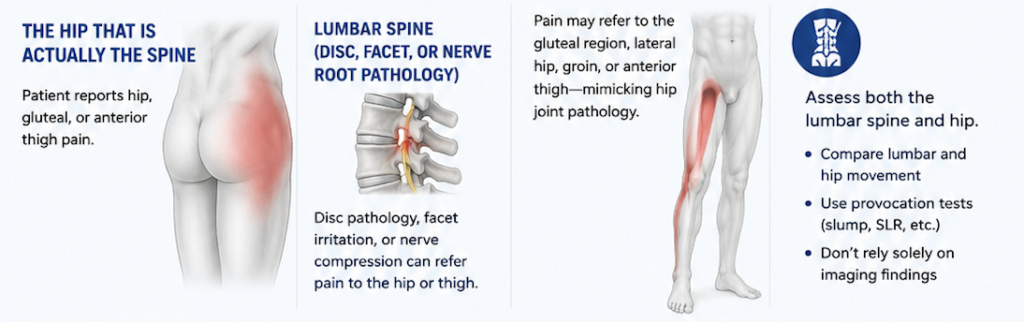
Patients with hip pain frequently present a diagnostic challenge. While groin pain often suggests intra-articular hip pathology, symptoms extending into the buttock, lateral thigh, or anterior thigh may originate elsewhere. Here is a list of potential causes of lateral hip pain:
- Greater trochanteric bursitis – pain with palpation posterior to the greater trochanter
- Gluteus medius tendonitis – pain with palpation on superior greater trochanter
- L4-L5 nerve root compression – provoked with SLR or slump test
- Piriformis trigger point – palpated midway between the SI joint and greater trochanter
- Quadratus lumborum trigger point – palpated between iliac crest and 12th rib
Lumbar radiculopathy, facet joint irritation, and spinal stenosis can all produce symptoms that mimic hip disorders.
Why does this matter?
Patients seek answers when they experience pain. Clinicians provide the greatest value when they look beyond the obvious. The next time a patient points to a painful shoulder, knee, or hip, remember that symptoms tell only part of the story.
The location of pain is where the conversation begins—not where clinical reasoning ends.
Understanding anatomy and referral patterns allows clinicians to uncover the true source of dysfunction, leading to more accurate diagnoses, more effective treatment plans, and ultimately better patient outcomes.
Join me next week as we examine another MSK clinical pear and take a deeper dive into the rotator cuff. It isn’t just about four muscles. I hope you join me.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








