Muscle Minute TUESDAY – A Wing Dinger, the Serratus Anterior

The name serratus anterior (SA) often conjures up images of scapular winging. Clinically, we often only consider this muscle if it is long/weak, causing scapular instability. But the intricate fascial connections and trigger points in this muscle are also problematic and understanding its multifaceted role in arm elevation is key. Let’s dive in.
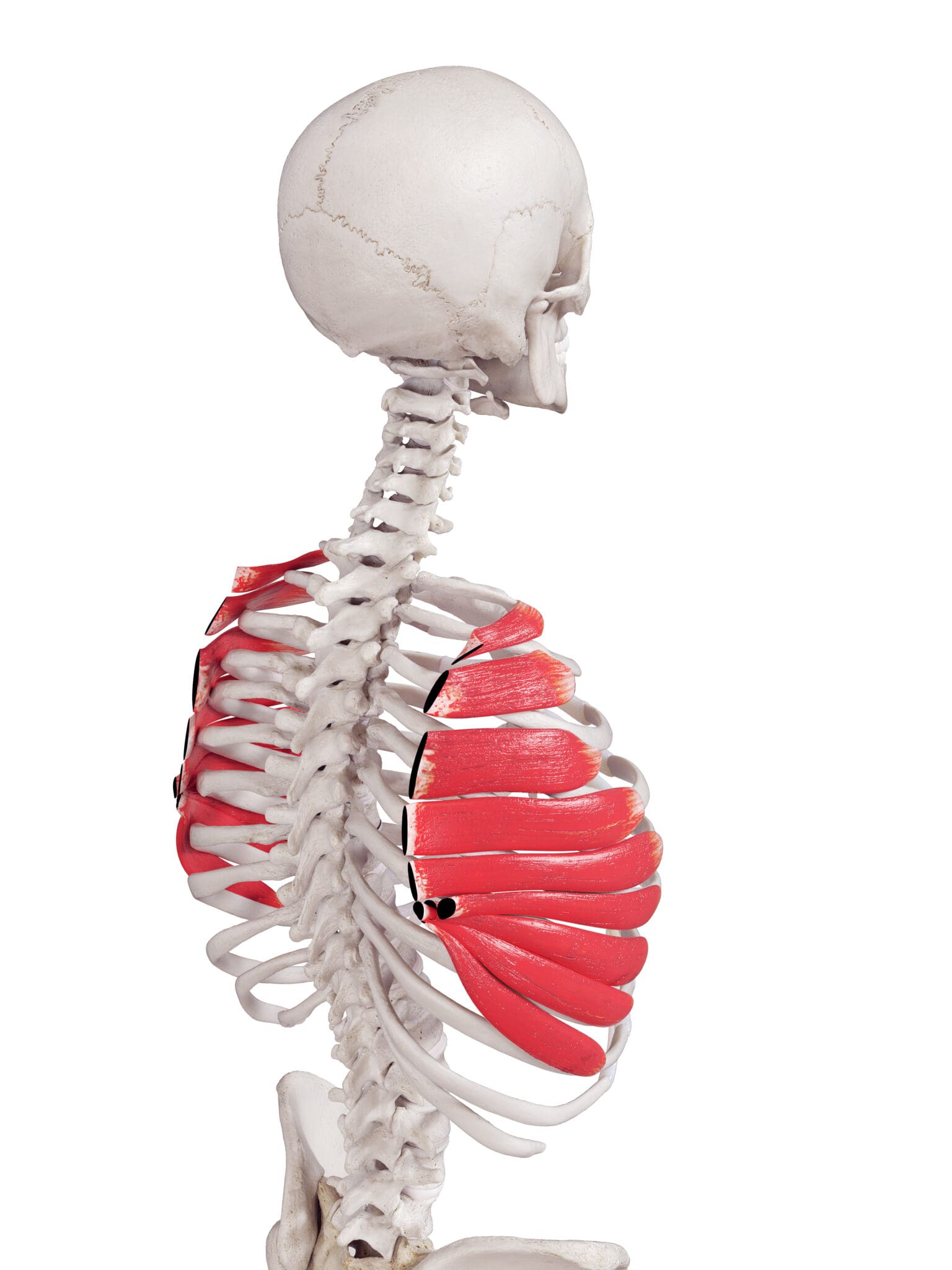
| Origin | upper portion of ribs 1-8 (or 9) |
| Insertion | costal aspect of medial border of scapula |
| Action | protraction, upward rotation, posterior tilt and external rotation of the scapula |
| Innervation | long thoracic n. (C5, C6, C7) |
| Antagonists | pec minor and rhomboid |
The Real World Serratus Anterior
Wait. You mean this muscle does more than just protract the scapula?! Yes. Check out that long list of actions. Posterior tilt and external rotation of the scapula are two of the motions responsible for opening up the subacromial space during arm elevation and these functions are made possible due to the attachment of the serratus anterior on the medial border of the scapula. Below is an excellent illustration of the intricate actions of serratus anterior. You can read more about it here.
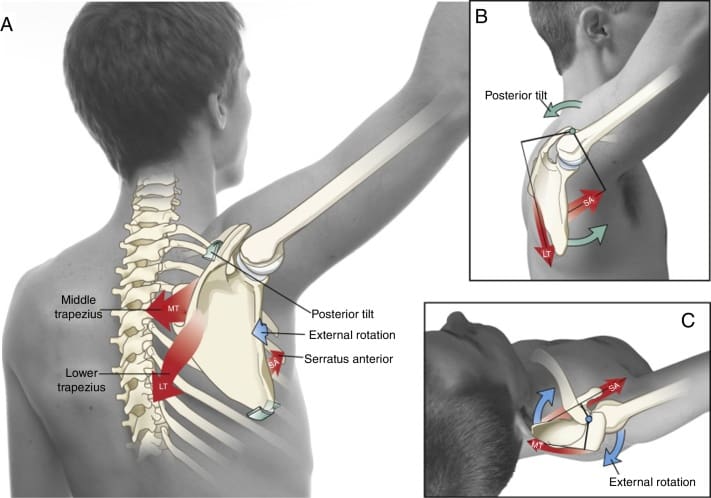
The serratus anterior is an integral player in the force couple of the scapula. When you lift your arm over your head, the humerus must upwardly rotate, along with the scapula. This is referred to as scapulohumeral rhythm. Each bone has a force couple that produces this rotation. For the scapula, the upper trapezius pulls up, the lower trapezius pulls downand the serratus anterior pulls forward. Coordinated activation of the all three muscles is requires for pain-free arm elevation.
Key antagonists of the SA are the pec minor and rhomboid, the former opposing posterior tilt function and the latter opposing the external rotation and protraction of the scapula. The serratus anterior also shares fascial connections with the rhomboid and external oblique. And a key functional synergist of the serratus anterior is the ipsilateral gluteus maximus. (I’ll talk more about this in a future blog)
The SA may also be affected by thoracic movement or posture. Picture yourself standing with your arms holding a stationary bar in front of you. Now, turn your body to the left. Can you see how left thoracic rotation may cause lengthening (weakening) of the right SA and shortening (trigger points) of the left SA?
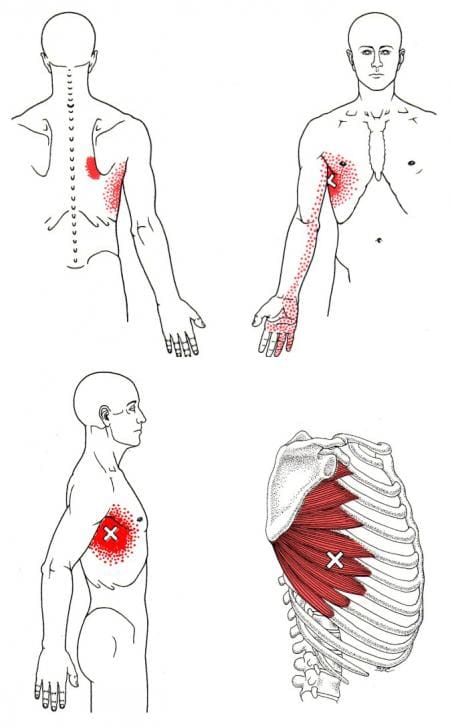
A an active trigger point of the serratus anterior will refer pain into the 4th and 5th digits of the hand, mimicking a C8 nerve root compression. It is the only scapular muscle to radiate pain into the distal upper extremity.
Here’s a short list of why this matters:
- If the serratus anterior is weak, the scapula will wing during the deceleration of arm elevation (deceleration of scapular retraction)
- Trigger points in the rhomboid or pec major may neurologically weaken the serratus anterior
- Serratus anterior weakness may be a cause of subacromial impingement
- In the scapular force couple, an imbalance of one of the muscle pulls causes scapular malpositioning. The most common pattern: a tight upper trapezius, a weak lower trapezius and a tight serratus anterior.
- Asymmetric thoracic rotation may cause SA weakening or shortening.
- Decreased functional rotation through the thoracic spine and ipsilateral hip may cause SA insufficiency.
- An SA trigger point may mimic cervical radiculopathy.
Conventional thinking says: A weak serratus anterior can cause shoulder impingement
Real World Thinking says: A weak or tight serratus anterior will affect arm elevation. Weakness is often due to postural asymmetry and or lack of mobility in the thoracic spine and ipsilateral hip. So don’t just do push-ups to strengthen this muscle. Consider thoracic and hip mobility and activation of the antagonists to restore normal function.
Phew! That was a lot. But thanks for considering all of this.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








