Anatomy TUESDAY – Clinical Anatomy Pearls 4 – Supraspinatus Tendon

When clinicians think of the supraspinatus, most remember the same anatomy lesson from PT school: “It initiates the first 15 degrees of shoulder abduction.”
While technically correct, this statement barely scratches the surface of the supraspinatus tendon’s true importance. In reality, the supraspinatus functions less like a prime mover and more like a dynamic stabilizer that allows the shoulder to move efficiently. Understanding its anatomy and biomechanics can dramatically improve the evaluation and treatment of shoulder pain.
The Anatomy Behind the Function
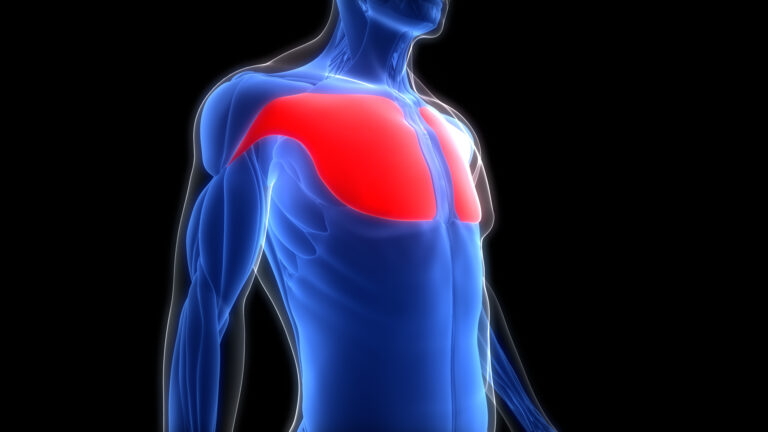
The supraspinatus originates from the supraspinous fossa of the scapula and travels laterally beneath the acromion before inserting onto the superior facet of the greater tuberosity of the humerus.
Unlike most tendons in the body, the supraspinatus passes through a relatively narrow space bounded by the acromion and coracoacromial ligmament (superiorly) and the humeral head (inferiorly).
This confined environment exposes the tendon to both tensile and compressive forces throughout shoulder motion. Few tendons in the body experience this combination of loading.
As the arm elevates—particularly into flexion and abduction—the tendon wraps beneath the coracoacromial arch and experiences compressive loading against surrounding structures. This has important rehabilitation implications.
Simply strengthening the tendon may not fully address symptoms if poor scapular mechanics or altered humeral head positioning continually increase compressive stress. Understanding both tensile and compressive loading encourages clinicians to think beyond isolated exercises.
The Real Job: Keeping the Humeral Head Centered
Many clinicians still describe the supraspinatus primarily as an abductor. While it certainly contributes to shoulder elevation, its more important role is maintaining glenohumeral stability.
As the deltoid contracts during arm elevation, it creates a strong superiorly directed force on the humeral head. Without restraint, the humeral head would migrate upward toward the acromion.
The supraspinatus—working with the infraspinatus, teres minor, and subscapularis—compresses the humeral head into the glenoid, creating a stable center of rotation. This dynamic compression allows larger muscles such as the deltoid to generate movement without sacrificing joint stability.
Think of the supraspinatus as the shoulder’s “precision stabilizer.” It doesn’t generate the most force, but it ensures that every degree of motion occurs around a stable joint.
Blood Supply Matters
Like many tendons, the supraspinatus has regions with relatively limited vascularity. Historically, the “critical zone” approximately 1 cm proximal to the insertion was believed to explain the high incidence of degeneration. But more recent studies suggest vascularity is more complex than originally thought.
Microvascular blood flow was highest at the musculotendinous junction and lowest at the lateral insertion. Healthy supraspinatus tendons had higher blood flow than pathological ones, with the lowest blood flow demostrated in those with subacromial impingement.
The Supraspinatus Never Works Alone
The supraspinatus is only one component of a highly coordinated movement system Optimal shoulder function depends on interaction among:
- Rotator cuff muscles
- Deltoid
- Serratus anterior
- Upper, middle, and lower trapezius
- Rhomboids
- Thoracic spine
- Rib cage
- Opposite gluteus medius/maximus
Weakness, delayed activation, fatigue, or stiffness in any of these regions may increase demand on the supraspinatus tendon. This explains why strengthening the cuff in isolation often produces incomplete results.
Assessment Pearls for the Supraspinatus Tendon
When evaluating patients with suspected supraspinatus pathology, resist the temptation to focus exclusively on special tests. Instead, evaluate the entire shoulder complex.
Ask yourself:
- Is the scapula rotating normally? (check strength of serratus anterior and lower trapezius)
- Does the thoracic spine extend and rotate adequately? (check side lying thoracic rotation and perform the thoracic sequence)
- Is the humeral head remaining centered during elevation? (check ability of infraspinatus and teres minor to depress the humeral head)
- Are the posterior cuff muscles providing balanced force? (check for trigger points in the infraspinatus and teres minor located in the posterior axillary region)
- Does the patient demonstrate adequate rotator cuff endurance rather than just strength? (is there pain with prolonged elevation?)
- Are symptoms primarily load-related, compressive, or both? (determine if pain occurs with manual muscle testing or if there is the presence of a painful arc)
- Why is the supraspinatus being overloaded? (check opposite gluteus medius and gluteus maximus strength)
These questions often reveal more than a positive empty can or full can test alone.
Why does this matter?
The supraspinatus is not simply the muscle that starts shoulder abduction. It is a dynamic stabilizer that helps center the humeral head, manages both tensile and compressive loads, and works in concert with the entire shoulder complex. When clinicians appreciate this broader role, they move beyond treating an isolated tendon and begin restoring efficient shoulder mechanics.
The most successful treatment plans don’t ask, “How do I strengthen the supraspinatus?” They ask, “Why is the supraspinatus being overloaded in the first place?” Answering that question often leads to more meaningful, long-lasting outcomes for patients.
Join me next week as we take a closer look at the patellar tendon.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]