
Muscle Minute TUESDAY – Medial Meniscus
I stumbled on an interesting study regarding meniscal tears in people aged 50-90. The study involved MRI scans of symptomatic right knees in 991 subjects. Here is what they found:
- Among those with x-rays showing osteoarthritis, meniscal tears were present in 63% of those with knee pain and 63% of those without symptoms
- 35% of the entire group presented with meniscal tears of the right knee (308 people)
- Of the 308 with meniscal tears, 66% were in the medial meniscus
Meniscal tears are often blamed on plant/pivot injuries, evoking images of athletes making rapid directional changes. But in my experience, most meniscal tears occur insidiously in the population mentioned: people who are doing a lot more sitting or walking than running at high speed in zig-zag fashion.
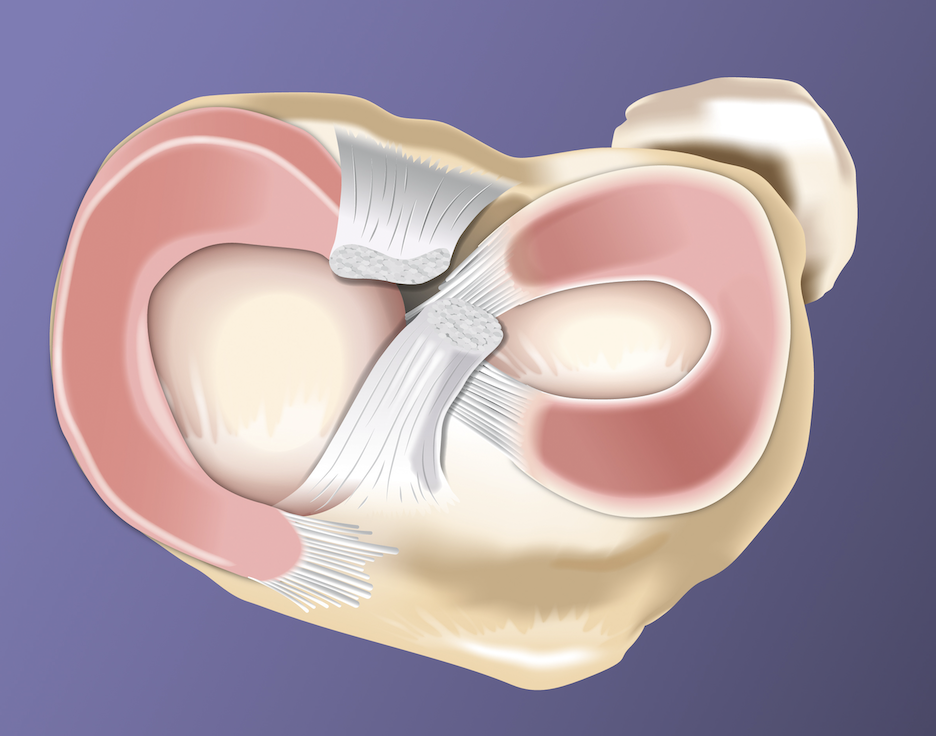
So how does the medial meniscus get in so much trouble? Let’s look at some anatomical facts:
- Medial meniscus is larger than the lateral meniscus and is tied down tighter with attachments to the medial collateral ligament (MCL) and the knee joint capsule
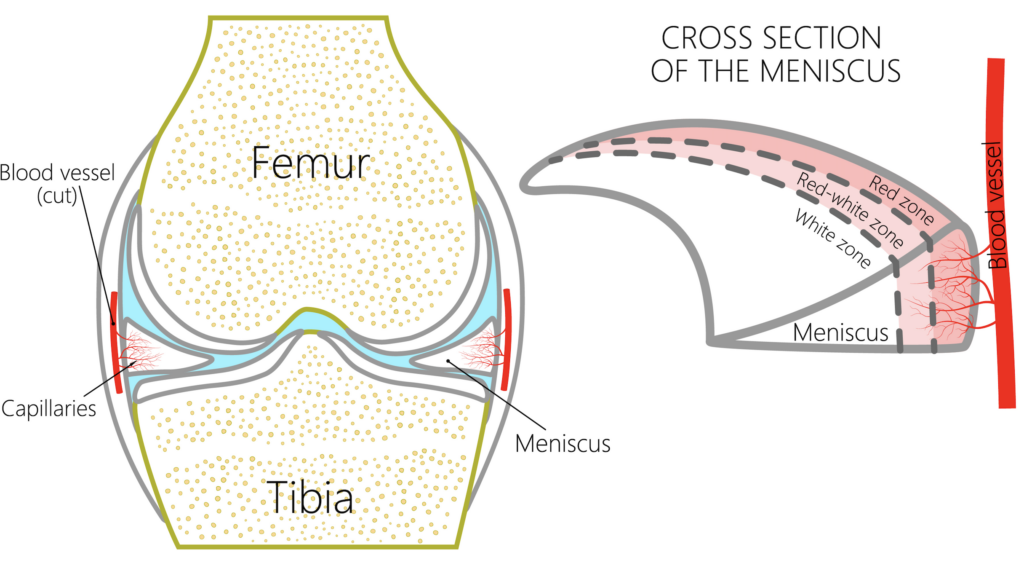
- The meniscii are pie-shaped, thinner towards the center and thicker on the periphery
- The inner portion of the meniscii does not have a blood supply (white zone), making this area unable to heal. Most tears occur in the white zone
When your foot hits the ground three things should occur to keep your meniscii happy: subtalar joint everts (foot rolls in), tibia internally rotates, femur internally rotates. This should happen like a chain reaction. One after the other. And as you push off, this process should reverse.
Pivoting isn’t bad for you…bad pivoting is bad for you (or your medial meniscus)
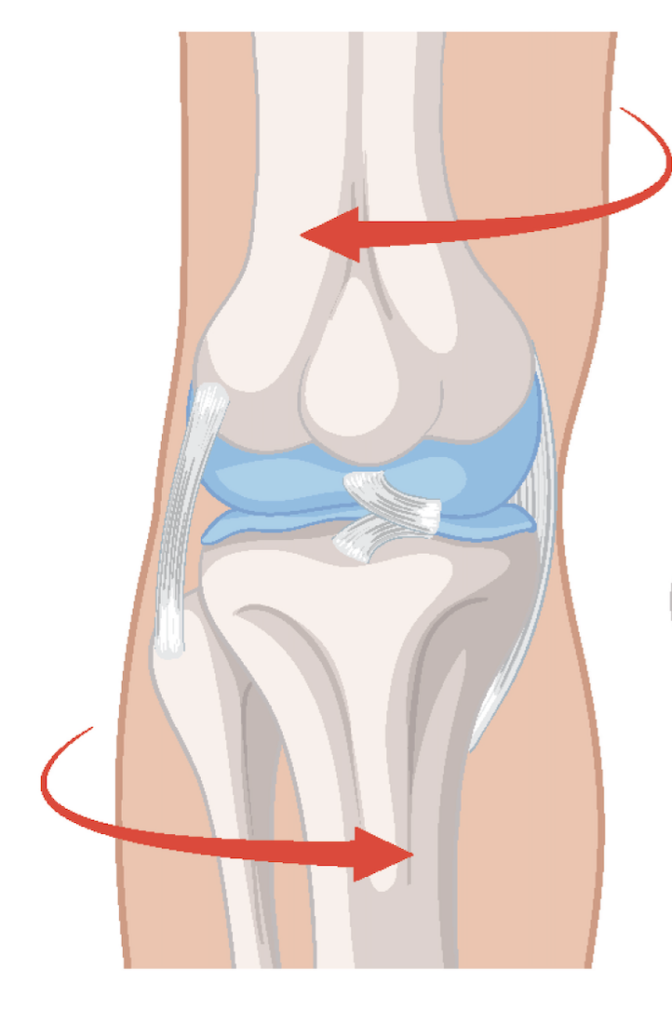
The picture above demonstrates a common abnormal rotational scenario. The tibia internally rotates and the femur does not OR the tibia stays internally rotated too long. This may occur with:
- Tightness of the hip external rotators (piriformis, posterior gluteus medius, adductor magnus, psoas major)
- Tightness of the medial hamstrings (semimembranosis, semitendinosis)
Try this test…
Do a standing quad set. You should be able to tighten your quadricep and NOT feel pain in the anterior knee joint line (front of the knee). If you feel a pinch in the front of the knee, chances are your meniscus is taking a hit. Here are some exercise ideas to fix it.
Why does this matter?
A mensicus tear is a lot like a hang nail. If you’ve ever had a hang nail, you realize it only hurts if it gets hung up on something. If it gets pesky enough, you fix it by trimming it off.
In the case of the meniscii, tears may be present even if your knee doesn’t hurt. That’s because most meniscal injuries occur over time, not just with a rapid plant and pivot move. Trimming a torn meniscus (partial menisectomy) may solve the “hanging up” issue, but it exposes the bone beneath it, potentially accelerating osteoarthritic changes in the joint.
So, test your standing quad set. Get rid of the pinch. Your medial meniscus will thank you.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








