Kinesiology THURSDAY – Nick’s Right Neck
That is not actually a picture of Nick, but he kind of looked like that. “I’ve been dealing with this pain for a couple of years,” he said, describing right cervical and scapular pain. He started serious weight training five years ago and for no apparent reason, his pain began. He describes deltoid pain so severe he was unable to lift anything at one point. He underwent PT involving scapular exercises for two months, but the most successful treatment was dextrose injections into the cervical region to expand the spaces for his nerves. This brought 1.5 months of pain relief.
MRI’s to his shoulder and neck were negative for rotator cuff tear but positive for degenerative changes in the cervical spine. He denies radicular symptoms into the upper extremities.
Here’s what I found…
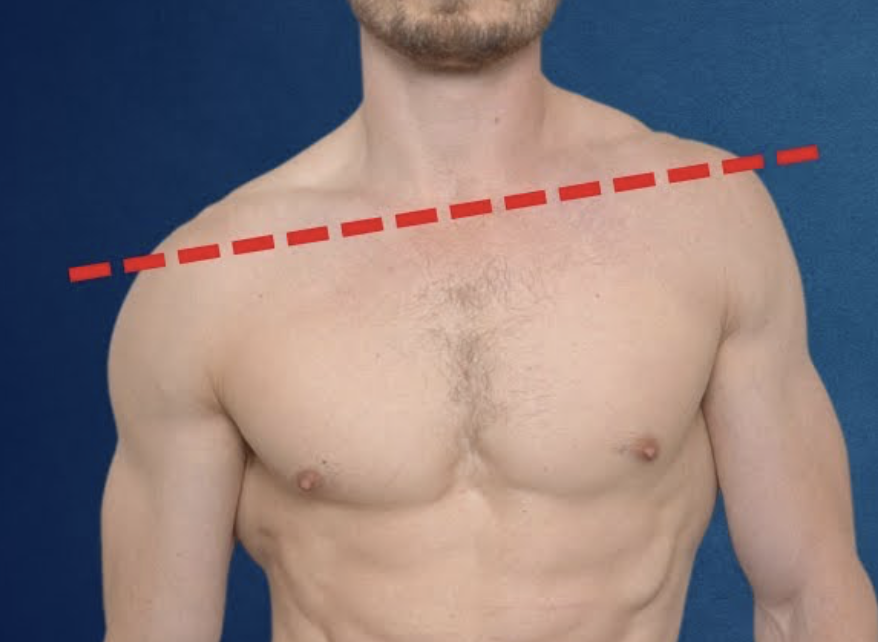
- Left shoulder was higher than the right (severe trigger point L upper trapezius)
- Cervical ROM was limited in flexion, extension, left side bend and left rotation
- Cervical MMT was 5/5 without pain provocation
- Upper extremity MMT 5/5 without pain provocation
- Cervical compression and distraction testing were negative
- No scapular winging noted
And then I looked further and here’s what else I found…
- Pelvic malalignment: R inflare, R posterior rotation, L on R sacral torsion
- Thoracic rotation limited R>L
- Severe hamstring tightness R>L
- Decreased B piriformis test (hip IR)
- Severe hypomobility R>L subtalar joint eversion
- Severe tightness of gastrocnemius (gravity drop test)
- Pelvis rotated to the right (determined by supine foam roll balance test)
The key thing to note above is how many things were tight on the right side that were nowhere near the cervical/scapular region.
The A in SOAP…
People have asked me how I can justify evaluating so many body parts when the diagnosis is for the neck. My initial thought, especially in cases like this where a localized evaluation does not give you an answer, is how can you not? We evaluate until we can come up with a plan. If I had to go off of just his cervical measurements, the only conclusion I would have drawn was his left upper trapezius tightness is somehow causing right shoulder pain and he has limited ROM that seems like his right levator scapula should have been the culprit.
When writing up my note, the A is key. S (subjective) stands for what the patient tells me. O (objective) is any data I pick up and there are no rules as to what data a clinician might measure. A stands for assessment or how I interpret all of that stuff in O. And P (plan) will be my plan that takes O and A into consideration.
Here was Nick’s A…
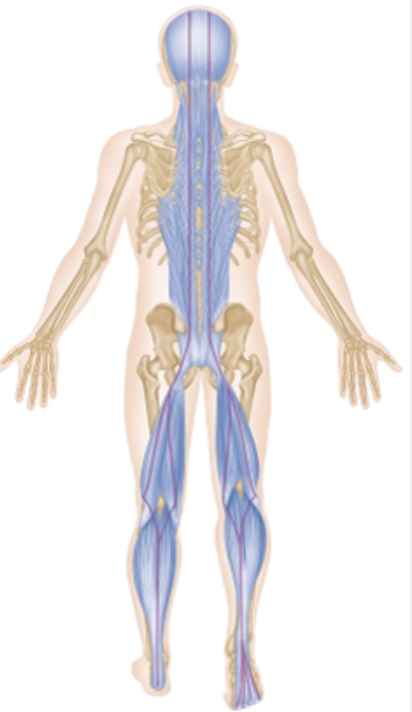
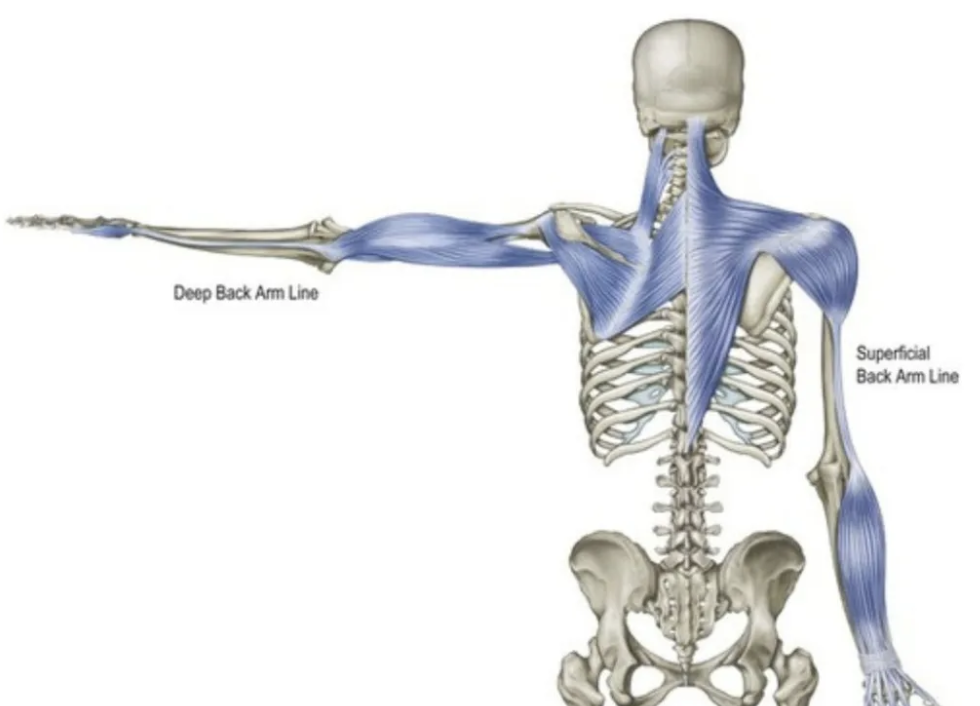
Myofascial pain syndrome affecting R upper quarter. Restrictions on superficial back line and back of arm line especially in the R LE contributing to R rotated pelvis and R scapular depression. L elevated from upper trapezius trigger point shoulder contributing to R upper trapezius strain/tension. Here’s are those lines for reference (we are all connected):
What I Am Going to Do:
I am going to fix what I found.
- Correct pelvic alignment
- Restore thoracic rotation with thoracic sequence
- Therapeutic exercises to promote hamstring and hip ER flexibility, correct R pelvic rotation and improve STJ eversion and ankle dorsiflexion
- Counterstrain the L upper trapezius
Why does this matter?
I wanted to share this case as an example of the importance of a biomechanical evaluation and taking a bigger look. Evaluate not just to pick up data but to find a real solution. Keep hunting the “O” until you get to an “A” and then put the plan in place.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]