Kinesiology THURSDAY – Market Vondrousova’s Left Knee

Markéta Vondroušová, a Czech professional tennis player ranked No. 6 in the world in singles by the WTA, just withdrew from the US Open with a left knee injury. The shot above was her last hit of the tournament (a forearm volley) and it occurred during a warm up session. She said it was an aggravation of an injury she felt in her prior match against Elena Rybakina three days ago.
No specifics were given about the injury, but injuries have plagued Markéta’s career including:
- September 2025: A knee injury forced a withdrawal from the US Open quarterfinal match.
- Early 2025: She experienced ongoing shoulder issues, leading to a break from the tour. She also withdrew from the Australian Open with a thigh injury.
- Late 2024: Underwent left shoulder surgery after the US Open.
- April-October 2022: A left wrist injury sidelined her for six months, requiring surgery.
- 2019: A left wrist injury led to the end of her season and subsequent surgery after Wimbledon.
- 2016: An left elbow injury ended her season in May.
She is a left-handed tennis player with a string of upper extremity injuries requiring wrist surgery in 2022 (to remove bone fragments from stress fractures) and shoulder surgery in 2024 (stated as a repair, but not specifically rotator cuff). And then in January, she withdrew from the Australian Open with a left thigh injury.
I found this headshot of her online:

Her left shoulder is significantly lower than her right. What does this have to do with her lower extremity? A higher shoulder is usually associated with a limb that is over supinating, while a lower shoulder is associated with a limb that over pronates.
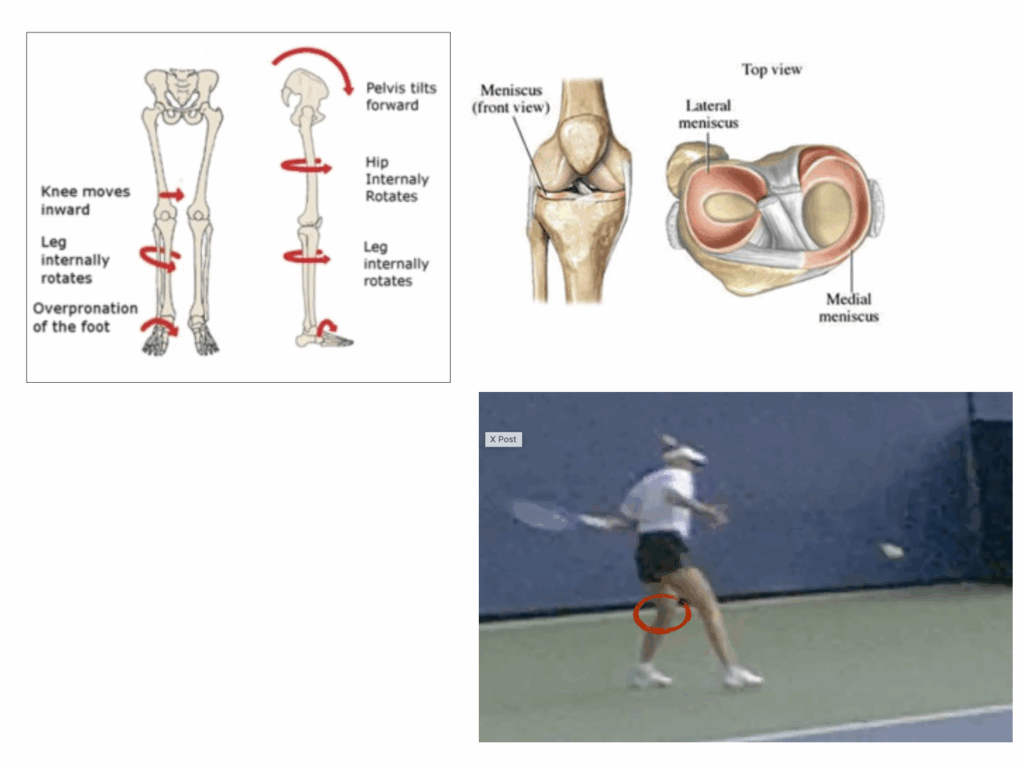
The forearm stroke requires loading of the ipsilateral leg. If a leg tends towards over pronation, this places muscles like the quadriceps, glutes and hamstrings in a long/weak position. If the large muscles of the leg/thigh are weaker, this predisposes her left knee to overuse rotational injuries such as meniscal tears and patellofemoral pain.
If you plant your left foot and pivot left, your tibia has to internally rotate to keep your big toe on the ground and effectively load your gluteus maximus. Tibial internal rotation would place stress on the anterior medial mensicus and posterior lateral meniscus. In the case of the patellofemoral joint, it would place stress on the lateral patellar facet. The illustrations below are of the right leg.
What would I do?
- Correct pelvic alignment.
- Check her right side for a cause of over supination (lack of subtalar joint eversion; psoas major trigger point, pelvic rotation to the right)
- Check her left side for common causes of over pronation (pelvic rotation to the right, weak gluteus medius, tight adductor, lack of ankle dorsiflexion)
- Check for trigger points that would predispose her to excessive tibial internal rotation or femoral external rotation (lateral gastroc, piriformis, medial hamstring, popliteus)
- Check thoracic rotation. Limitations for thoracic rotation include tight latissimus dorsi, hypomobile thoracic segements (usually between T3-T6)
- Check ability for left hip to externally rotate (FABER test)
And I would fix what I found.
I’m not sure if all of Markéta Vondroušová’s upper extremity injuries stemmed from the forehand stroke, but her knee injury did this time. And reaching to the left in the forehand stroke requires loading of the left leg. If you play or know someone who is injured from playing the game, assessing when the injury is most problematic may be helpful. Forehands are driven from the same side leg while backhands are powered by the opposite leg. Solving an abnormal rotational scenario at the knee by assessing joints above and below is key to stopping repeated aggravation of soft tissue.
Because nobody has time to be in pain. Especially at the US Open.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








