
Anatomy TUESDAY – Clinical Anatomy Pearls 2 – The Rotator Cuff
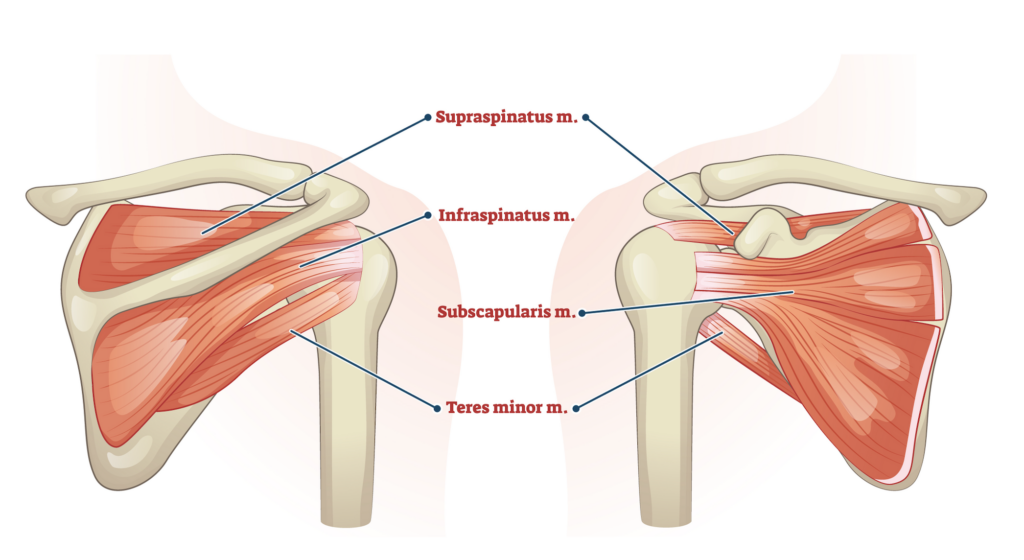
Ask any musculoskeletal clinician to name the rotator cuff muscles, and the answer usually comes quickly: Supraspinatus, Infraspinatus, Teres Minor, Subscapularis (SITS)
For many healthcare professionals, this list represents the extent of their rotator cuff anatomy knowledge. Yet understanding the rotator cuff as simply four muscles responsible for shoulder movement misses its most important clinical function.
The rotator cuff is not just a collection of muscles—it is a sophisticated dynamic stabilization system that allows the shoulder to remain both mobile and functional.
For clinicians treating shoulder pain, appreciating this distinction can significantly improve assessment, clinical reasoning, and treatment outcomes.
The Shoulder Stability Challenge
The glenohumeral joint is often described as a golf ball sitting on a tee, with the humeral head being 4x the size of the glenoid fossa. During motion, only 25% of the humeral head comes in contact with the scapula at any given movement. This design provides extraordinary mobility at the cost of inherent stability, dependent on soft tissues to maintain joint integrity during movement.
Most anatomy textbooks focus on the movement actions of the cuff muscles:
- Supraspinatus: abduction
- Infraspinatus: external rotation
- Teres minor: external rotation
- Subscapularis: internal rotation
While technically correct, these descriptions fail to capture the cuff’s true importance.
Here is a more accurate list:
- Supraspinatus – acts as a vertical “steerer” pulling the humeral head superiorly
- Infraspinatus – prevents excessive posterior migration of the humeral head
- Teres minor – prevents excessive posterior migration of the humeral head
- Subscapularis – prevents excessive anterior migration of the humeral head
The rotator cuff functions primarily as a dynamic stabilizer, compressing the humeral head into the glenoid fossa. This compression creates a stable center of rotation that allows larger muscles to generate movement efficiently. Without this stabilizing force, the humeral head may migrate excessively, altering joint mechanics and increasing stress on surrounding tissues.
In other words, the rotator cuff provides control before it provides motion.
One of the most clinically relevant concepts in shoulder anatomy is the idea of force couples. A force couple occurs when muscles generate opposing but coordinated forces that create controlled movement and stability.
Coronal Plane Force Couple
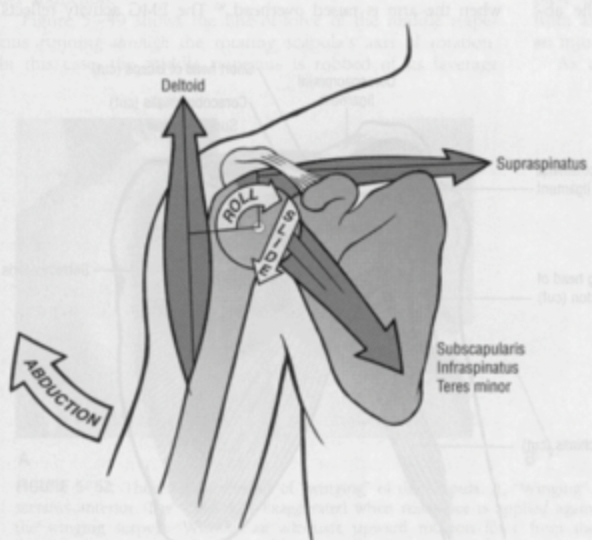
The deltoid produces a strong superiorly directed force during arm elevation. If unopposed, this force would cause excessive superior migration of the humeral head. The rotator cuff (ITS) counters this action by producing a compressive and inferiorly directed force that helps maintain joint centration.
This balance allows smooth, pain-free elevation.
Transverse Plane Force Couple
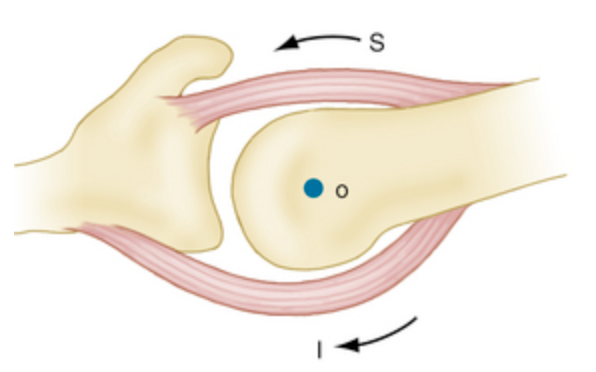
The subscapularis (S) anteriorly and the infraspinatus/teres minor (I) posteriorly create balanced forces around the humeral head. Together, they stabilize the shoulder during rotational movements and dynamic activities.
Disruption of either force couple can contribute to altered movement patterns, weakness, and pain.
Why Weakness is Not Always the Problem
Tears will occur in muscles that are weak, but often in stabilizing muscles like the rotator cuff, the weakness is produced by the muscle being in a long/weak (neurologically inhibited) position at rest.
Look at this picture closely:
- Supraspinatus (the most commonly injured rotator cuff muscle) is placed in a long/weak position if the scapula is upwardly rotated (upper trapezius trigger point)
- Infraspinatus/teres minor become short/tight in an upwardly rotated scapula
- Subscapularis may become long/weak with trigger points in infraspinatus/teres minor
- Infraspinatus (second most commonly injured rotator cuff muscle) becomes long/weak with trigger points in the subscapularis)
- An elevated scapula creates shortening of the upper trapezius also resulting in scapular upward rotation
- A protracted scapula causes trigger points in the infraspinatus/teres minor and creates anterior migration of the humeral head
In other words, often the fix to rotator cuff weakness is NOT this:
The fix to neurological inhibition of the rotator cuff and its ability to stabilize is often in correcting scapular position by:
- Normalizing thoracic mobility
- Eliminating forward head posture
- Activating the lower trapezius (to counteract upper trapezius tightness)
- Releasing trigger points in antagonists of the injured muscle
Why does this matter?
The rotator cuff is far more than four muscles that move the shoulder. It is a highly coordinated stabilization system that works alongside the scapula, thoracic spine, nervous system, and larger shoulder musculature to create efficient movement.
When clinicians shift their perspective from “Which rotator cuff muscle is injured?” to “How is the entire shoulder system functioning?” assessment and treatment become more effective. Understanding the functional anatomy of the rotator cuff allows clinicians to move beyond simplistic diagnoses and develop interventions that address the true drivers of dysfunction.
Remember, the rotator cuff’s most important role is not producing movement—it’s controlling movement. By viewing the cuff as a dynamic stabilizer rather than simply four isolated muscles, clinicians can improve clinical reasoning, rehabilitation strategies, and patient outcomes. Consider the Cuff.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








