Kinesiology THURSDAY – Agonist v Antagonist (The Tug-O-War Series)
I want to kick off a series on the battle between functional agonists and antagonists. It shouldn’t be a battle, but often in chronic pain and injury there is an imbalance between two opposing muscles and in that imbalance lies the secret to getting rid of pain and restoring movement.
Common agonist/antagonist relationships consider movement primarily in one plane (i.e. quadriceps v. hamstrings). But most muscles are triplanar, performing or assisting in actions in the sagittal, frontal AND transverse planes of motion. A functional antagonist is a muscle that performs an action opposite of the agonist in ANY plane of motion. The solutions to many chronic overuse injuries lies in understanding these less often considered relationships.
In the next 10 weeks, we will dive into common, but not often considered, functional tug-o-wars. Each Thursday, you will learn about:
- The functional relationship of two muscles
- Common injuries that occur if the relationship is imbalanced
- How to fix the imbalance with manual therapy and/or exercise
First, we need to lay some groundwork. Here are the underlying principles behind functional tug-o-wars:
- Reciprocal innervation (the inhibition response): A shortening contraction elicited by the alpha motor neuron results in excitation of the Ia inhibitory motor neuron to the opposing muscle. For example, the concentric contraction of the gastrocnemius elicits an inhibitory response in the tibialis anterior. This is a normal response.
- Muscle spindles are located in the muscle belly, detect rate of stretch and elicit a muscle contraction. This is a normal response.
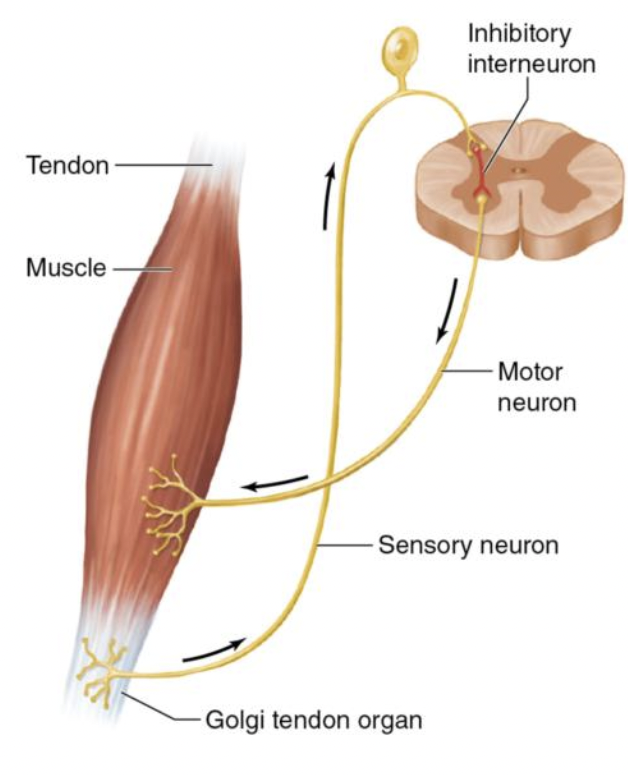
- Golgi Tendon Organs: Located in the musculotendinous junction gauge tension and elicit muscle inhibition This is a normal response.
- The Gamma System: The regulatory system that innervates the intrafusal muscle fiber at the ends of the muscle spindle. Determines “normal” length of a muscle by adjusting the sensitivity of a muscle spindle. If sensory input is limited (from chronic shortening), the gamma system threshold is lowered, creating abnormal muscle response and resultant trigger points.
- Trigger Points (TrP) Hyperirritable palpable nodules located in a taut band of skeletal muscle. A signal of an overactive muscle spindle. Usually occurring in muscles that are chronically short.
- Muscles that cry out in pain are long/weak, neurologically inhibited and unable to tolerate normal stress. – LISTEN TO THESE
- Muscles that are short/tight are neurologically overstimulated, creating an inhibitory response in an antagonist – TREAT THESE
That was a lot. If you made it this far, then you have done the hard part. Next week, we’ll start the fun part and kick things off with the bicep femoris v peroneus longus tug-o-war, one of the most common causes of recurrent ankle sprains.
Are you excited? I am. If you are a clinician, it will open your eyes to the possibilities of treating chronic injury. If you are a non-clinician dealing with a pain issue, it will give you hope that there is an answer to your problem even if sophisticated testing has not given you answers.
It will take a little brain work, just like understanding the concepts above. But understanding these relationships will pay dividends in solving complex orthopedic problems.
Take a deep breath…here we go.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]