
Kinesiology THURSDAY – Nathan Eovaldi’s Right Shoulder

Texas Ranger All-Star pitcher, Nathan Eovaldi, is likely done for the season with a reported right rotator cuff strain. He just pitched nine strikeouts in seven innings against the Guardians on August 22 and noticed soreness in the shoulder over the next couple of days. He shut down his bullpen session yesterday when the pain persisted. An MRI confirmed a rotator cuff strain. He is currently being placed on a 15-day injury list, but best season of his career is likely over.
Note: In June, he was limited to one game due to a right elbow injury (overuse). He has a history of two Tommy John surgeries to repair a partially torn ulnar collateral ligament (UCL) and common flexor tendon (medial elbow), in 2007 when he was in high school and in 2016 when he played for the Yankees.
Most pictures of him online show him throwing, but I found this headshot of him. Notice his right shoulder is slightly lower and more protracted than his left. How could this contribute to his rotator cuff strain?
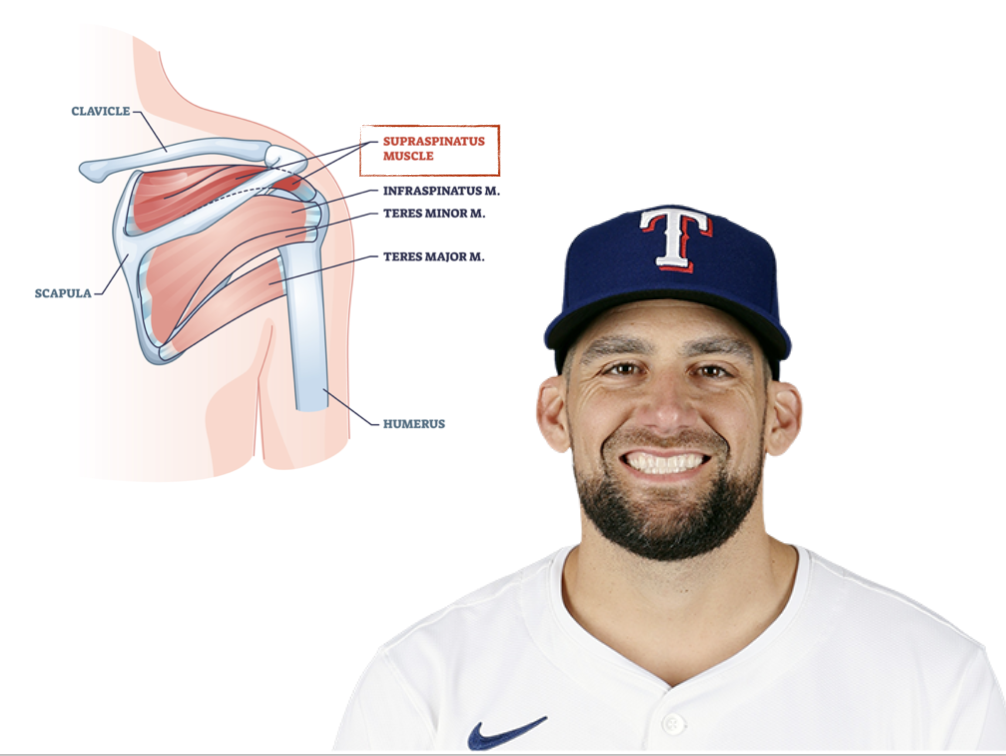
The news reports did not specify which rotator cuff muscle was strained but the most commonly sprained muscle is the supraspinatus. Let’s take a look at how the supraspinatus would be affected with a downwardly rotated scapula.
With the arm at your side, the supraspinatus should be virtually silent. But this is dependent on several factors, one of which is a slight upward rotation of the scapula. If the scapula is in the proper position, the humeral head rests on the glenoid fossa. If the scapula is downwardly rotated, this requires the supraspinatus to be constantly active to stabilize the humeral head in the socket. It’s like the humeral head got the chair pulled out from underneath it. That’s a lot of work for a small muscle in addition to stabilizing the humeral head during throws that average 94.1 mph. A recipe for an overuse scenario.
Trigger points that indicate a downwardly rotated scapula:
- pec minor (downwardly rotates and protracts the scapula)
- rhomboid (downwardly rotates and retracts the scapula)
Most likely, the pec minor is contributing to his situation. But these kind of problems are rarely just due to one muscle. Check out his injury history:
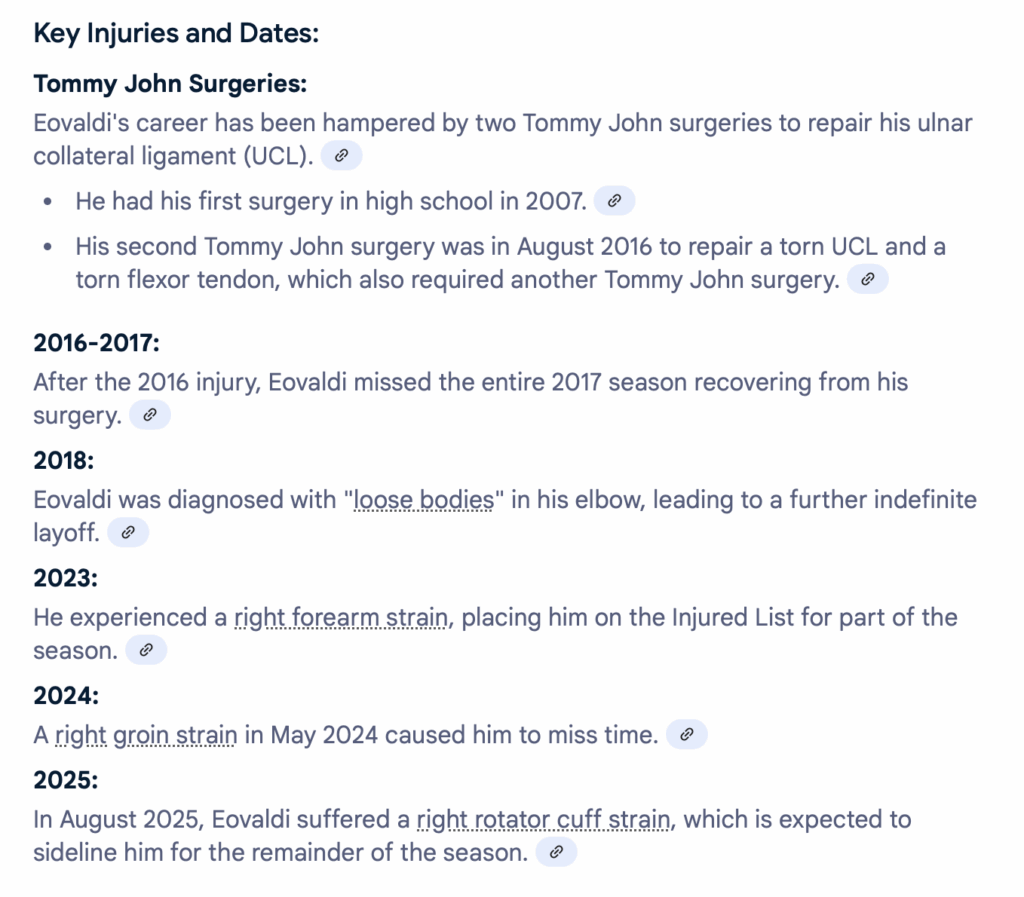
The list above fails to mention a right calf strain (2020) and the recent elbow strain (June 2025). All of these injuries, including the lower extremity injuries, indicate difficulty with the loading phase of the pitch.
What would I do?
If I was charged with getting Nathan back on the mound in 15 days, this is what I would do:
- Correct pelvic alignment
- Check for the ability of his right hip to rotate (FABER and piriformis test)
- Check side lying thoracic rotation and correct with the thoracic sequence
- Check to see if his right shoulder is lower because his LEFT shoulder is higher. This could be the case if he has trigger points in the LEFT quadratus lumborum and upper trapezius
- Check for trigger points in the right pec minor
- Check for mobility of his right ankle (dorsiflexion and eversion)
- Check for clavicular subluxation at the sternoclavicular joint
And I would fix what I found.
Why does this matter?
Maybe this information gets into the hands of the people working with Nathan, but his scenario is common in throwing athletes. When we evaluate a shoulder, it’s important that we don’t just stop with the tests that tell us “what” is happening (MMT to the rotator cuff, special tests, ROM). In the case of overuse injuries, the small muscles are likely strained because other things aren’t contributing. Our evaluation MUST include information that tells us the “why” of the injury.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








