
Kinesiology THURSDAY – The Sternoclavicular Joint and Arm Elevation
And, we’re back! After a short hiatus to visit Austria, the land of the Sound of Music and the birthplace of Mozart (which I highly recommend), I return renewed and excited to resume the exploration of the human body. And there is no better place to start than the only boney attachment of the entire upper extremity to the core of the body, the sternoclavicular joint (SCJ).
Kinesiology of the clavicle with arm elevation:
- From 0˚-90˚ of arm elevation, the clavicle upwardly rotates with its axis at the SC joint until the costoclavicular ligament becomes taut. This causes the scapula to upwardly rotate 30˚.
- From 90˚-180˚ arm elevation, the clavicle rotates posteriorly on its longitudinal axis with its movement centering around the acromioclavicular (AC) joint. This causes the scapula to upwardly rotate an additional 30˚.
When things go wrong:
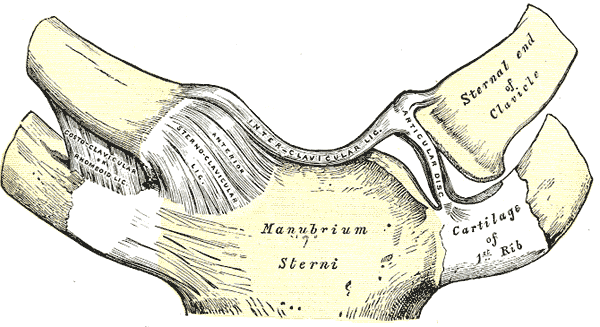
This SCJ is a saddle joint that is often overlooked in evaluation of shoulder and neck dysfunction. It is a major contributor in arm elevation and horizontal abduction/adduction and has key muscle attachments:
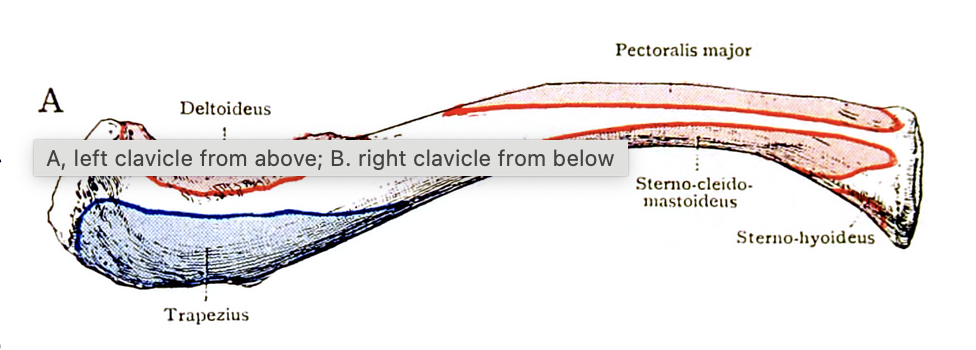
This is the left clavicle viewed from above. Notice the tug-o-wars that may occur in the functional antagonistic relationships of the pectoralis major v SCM and the anterior deltoid v upper trapezius. Remember, when it comes to antagonists, if one muscle is short/tight, the other is long/weak.
It is not uncommon to see upper trapezius and pectoralis major tightness in patients with painful or limited arm elevation. Picture that scenario acting on the clavicle pictured above. These two muscles act as a force couple on the clavicle with tightness creating a pull that would cause:
- anterior migration of the medial clavicle
- posterior migration of the lateral clavicle (AC joint)
- weakness of the anterior deltoid (a prime mover in shoulder flexion)
How do you test this?
Reach overhead with one arm. Do you feel a pinch at the top of your shoulder?

If you are a clinician checking this on a patient, have them perform active supine shoulder flexion with the elbow locked in extension (straight arm). Ask them where they feel it. If a pinch is felt in the superior shoulder, then assess the medial clavicle for posterior or anterior subluxation.

Try this simple fix for an anteriorly displaced medial clavicle, the most common subluxation associated with shoulder impingement.
Why does this matter?
Shoulder impingement is one of the most common overuse injuries of the shoulder, often involving rotator cuff tendonitis and irritation and painful arm elevation. Understanding the role of the sternoclavicular joint in arm elevation is key in solving this problem. If you can clear impingement of the shoulder with the patient in supine, any exercises performed to strengthen the shoulder will be more effective.
So, don’t overlook this tiny but significant joint. Assess it and fix what you find.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








