
Kinesiology THURSDAY – The Why Behind Patellofemoral Pain

One of the most common overuse injuries in orthopedics is patellofemoral pain (Runner’s knee), pain underneath the knee cap that often worsens with squatting, going up and down stairs and prolonged sitting. If you squat and your knees are “noisy”, chances are you are experiencing abnormal pressure under the patella.
Conventional treatment often generally includes strengthening of the quadriceps and ensuring proper flexibility of the hip muscles to normalize tracking of the patella. But understanding the complexity of this joint will lead one to even better solutions. Let’s get started.
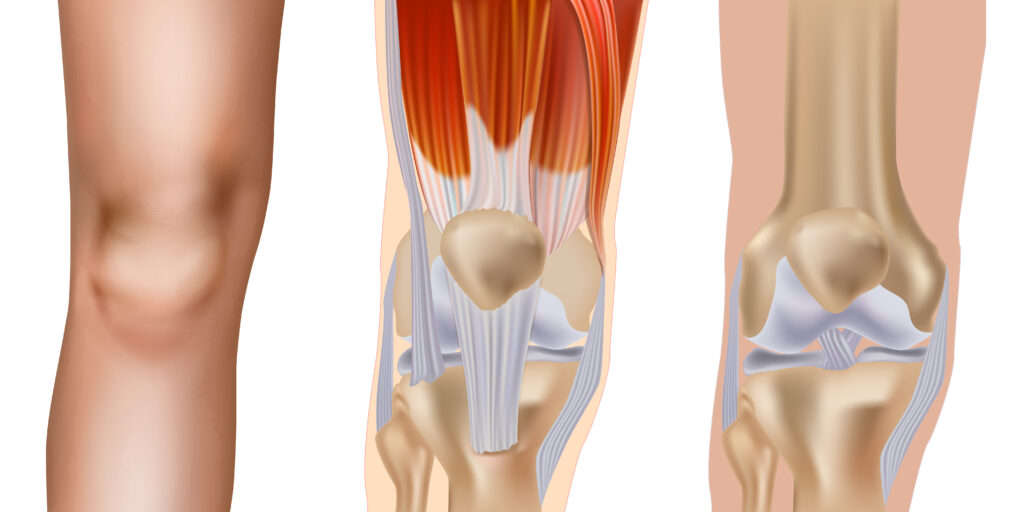
The patella is in a unique position in that it sits between the femoral condyles (femur) but is attached to the tibial tuberosity (tibia). The femur is controlled by the hip joint and the tibia is controlled by the ankle.
KinKNEEsiology…
When the foot hits the ground, or when you squat or climb stairs, the tibia internally rotates causing the patella to move medially. The femur also internally rotates which moves the medial femoral condyle out of the way. This movement of the femur and tibia eccentrically load the biggest muscles of your body, the quadriceps, gluteus maximus and hamstrings, in preparation for pushing off. During the push-off or concentric phase the motions of the tibia and femur are reversed as the tibia externally rotates, the patella moves laterally and the femur also externally rotates.
When things go wrong…
- Foot hits the ground and tibia does not internally rotate – occurs if the subtalar joint does not evert or the lateral hamstring is tight. This results in medial patellofemoral pressure. The FIX: mobilize the subtalar joint and stretch the lateral hamstring with the revolving triangle.
- Foot hits the ground and femur does not internally rotate (most common) – occurs with tightness in the deep external rotators of the hip and/or lateral gastroc. Trigger points may be present in the following: psoas major, piriformis, posterior gluteus medius, vastus lateralis, adductor magnus and lateral gastrocnemius. This results in medial patellofemoral pressure. The FIX: Release trigger points and prescribe stretches for the tight muscles. The most common stretch to fix this problem is the pigeon pose.
- Push-off and tibia does not externally rotate – occurs if the medial hamstring or graciilis muscle (adductor) is tight. This results in lateral patellofemoral pressure. The FIX: triangle pose and sumo squats
- Push-off and femur does not externally rotate – occurs is gluteus medius and gluteus maximus are weak. This results in lateral patellofemoral pressure. The FIX: Strengthen the gluteus medius with mini-band lateral stepping or side planks. THEN strengthen the gluteus maximus in the sagittal plane first and then advancing to the transverse plane. (hip hinging, lunging and then lateral low rows or woodchoppers)
How do you know if it’s the medial or lateral patella causing pain? Palpate it.
Why does this matter?
Solving patellofemoral pain is more than just about strengthening the quad and stretching the hamstrings. The position of the patella makes it dependent on hip and ankle mobility and timing to ensure pain-free function.
Though patellofemoral pain appears with movements in the sagittal plane, often the cause lies in the transverse or frontal plane. Assessing for one of the most common abnormal scenarios above will lead you to an efficient and effective solution. It’s worth a look.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








