Muscle Minute TUESDAY – Meet the Vastus Lateralis

I can’t believe it’s taken me this long to write about this muscle. I deal with it every day and maybe you do too. Or you should. Have you ever rolled out your IT bands? Chances are you were rolling out trigger points in the large muscle underneath the ITB, the vastus lateralis.
As the largest of the four quadricep muscles, the vastus lateralis (VL) not only helps extend the knee, but by virtue of its attachment to the lateral patella, it exerts influence on the hip joint without even crossing it. Let’s dive in.
| Origin | greater trochanter, intertrochanteric line, gluteal tuberosity, linea aspera (femur) |
| Insertion | lateral border of patella, quadriceps tendon, patellar tendon, small slip into distal ITB |
| Action | knee extension, patellar lateral glide, deceleration of femoral internal rotation |
| Innervation | femoral n. (L2, L3, L4) |
| Antagonists | bicep femoris, VMO |
The Real World Vastus Lateralis
Wait. This muscle is an external rotator of the hip?! Kind of. When the foot hits the ground and the tibia internally rotates, the femur also internally rotates. This causes the lateral femoral condyle to come in contact with the lateral patella, and the VL exerts a force to eccentrically control femoral internal rotation and then concentrically contracts to externally rotate the femur.
Pretty wild that a muscle that doesn’t even attach above the hip can rotate the hip. Evidence of this action can be seen in the prevalence of trigger points in this muscle. Remember, trigger points set up in muscles that are chronically short. If all this muscle did was extend the knee, then trigger points would indicate people are walking around with hyperextended knees. But this is not the case.
What we often see is trigger points in this muscle in people who have a tightness in other hip external rotators (piriformis, post gluteus medius, psoas major, etc.). And we rarely see trigger points in its counterpart, vastus medialis. Here’s a trigger point chart:
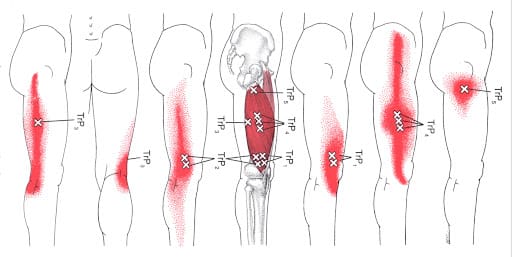
TrP4 looks a lot like the ITB, doesn’t it?
A compelling study showed that VMO was activated more than VL when standing on uneven surfaces (in this case an inflated disc) versus on stable ground, a move that requires more subtalar joint eversion (pronation). So if you want the VMO to fire more than the VL, perform lower extremity activities on unstable surfaces.
Here’s a short list of why this matters. A tight vastus lateralis:
- May limit hip internal rotation, causing an over supination of the lower limb (lateral knee, lateral ankle and medial hip soft tissue stresses)
- A tight vastus lateralis may inhibit the VMO, a commonly weak muscle following knee surgery. Working on balance on uneven surfaces may reverse the abnormal ratio of VL/VM activation.
- If it feels tight to roll your ITB, remember it’s probably your vastus lateralis, which means you should be stretching to improve hip IR (pigeon pose), or squatting with your feet and knees together to improve the flexibility of this muscle (versus the standing side bend ITB stretch). This is a great example of stretching other muscles to get one to relax.
Conventional thinking says: The vastus lateralis extends the knee.
Real World Thinking says: The vastus lateralis slows down or prevents femoral internal rotation and then externally rotates the femur as it extends the knee. If tight, it becomes problematic as it causes an over supination reaction of the lower extremity. Tightness in this muscle may also inhibit VMO contraction. Instead of just rolling it out, work to improve hip internal rotation and pronation if the vastus lateralis is tight. Think differently about the vastus lateralis.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]