
Kinesiology THURSDAY – Gunnar Hoglund’s Left Hip Impingement

Gunnar Hoglund, 25-year old starting pitcher for the Oakland Athletics finally made his MLB debut on May 2, 2025. His first game, he struck out 8 batters. On May 31, he gave up 8 runs on 10 hits against the Blue Jays and that is when he felt his left hip pain and was diagnosed with hip impingement. He was placed on a 15-day injury list. It was just announced that he will miss the rest of the 2025 season after undergoing successful left hip labral repair.
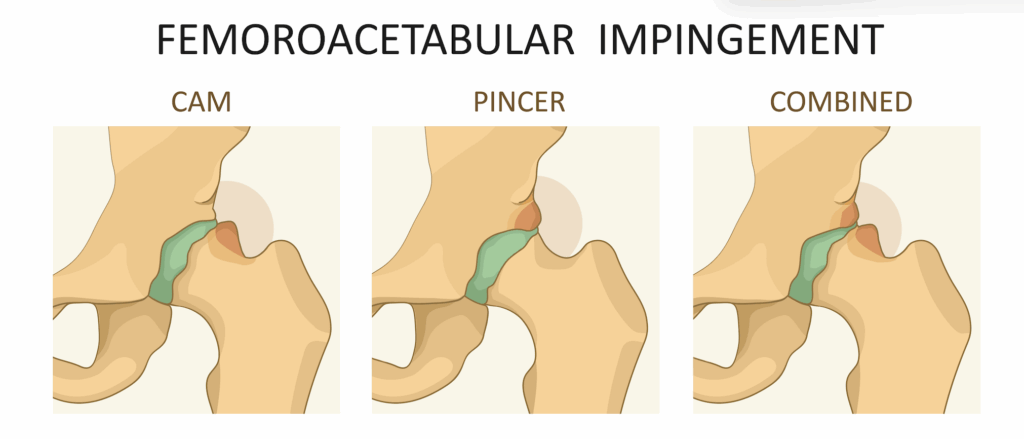
Hip impingement is usually felt as a pain in the groin in end ranges of flexion and internal rotation. Though impingement is usually classified as pincer (excessive bone on the acetabulum) or cam (excessive bone on the femur), impingement of the labrum is what ultimately causes a tear.
In the case of Hoglund’s left hip, the deceleration of his pitch requires significant amounts of flexion and internal rotation with the knee extended. Knee extension decreases the amount of rotation that occurs at the knee, creating greater rotational load on the hip joint.
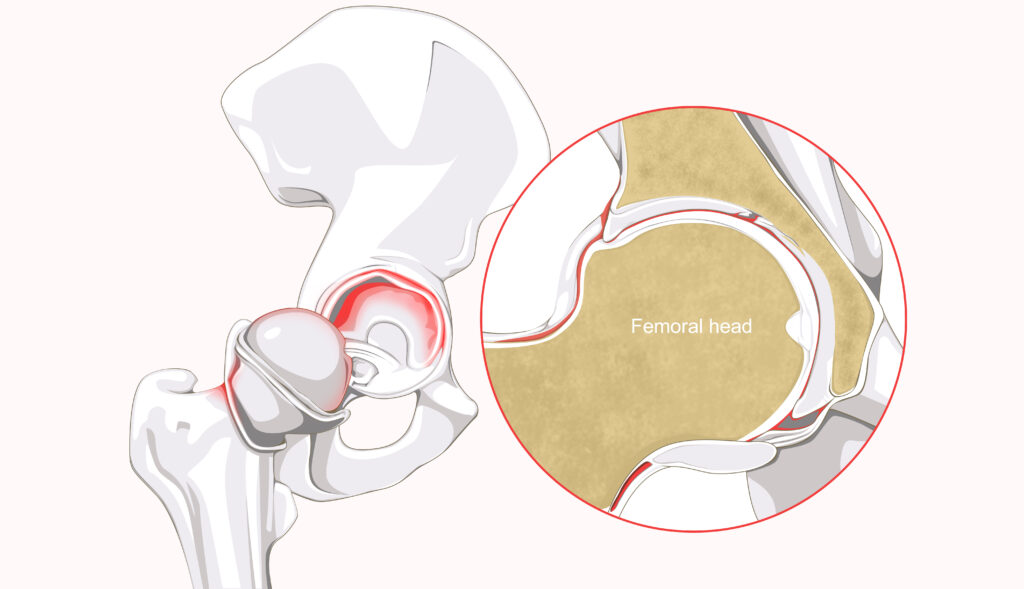
HIp impingement occurs when, at rest, the hip is sitting in a slightly abnormal position. Normal hip flexion and internal rotation mechanics require the femoral head to glide posteriorly. From a biomechanical standpoint, a femoral head sitting slightly anterior at rest would predispose one to anterior impingement of the hip during flexion and internal rotation. Additionally, excessive hip adduction (from lack of gluteus medius stabilization), may predispose one to superior hip impingement. It isn’t uncommon to see a compensatory increase in hip adduction when there is a limitation in hip internal rotation.
Here’s a list of things that may place the femoral head in a slightly anterior position at rest:
- Innominate inflare
- Toe-out walking or standing
- Trigger points in the following muscles:
- Posterior gluteus medius or piriformis
- Vastus lateralis
- Adductor magnus
- Psoas major
- Lateral gastrocnemius
What Would I Do?
I would test hip rotation with a simple cross-legged test:


You should be able to do both without feeling a jam in your hip. If you did, this is how I would treat you (and Hoglund).
- Correct pelvic alignment
- Palpate for trigger points in the list above and release what I found
- Test for gluteus medius strength
- Strengthen gluteus medius to stabilize against excessive hip adduction AND then
- Strengthen the gluteus maximus to decelerate functional hip internal rotation, first allowing the knee to flex and then with the knee extended.
Hip impingement is more common than people think. A lot of people just deal with it over years. Fixing the impingement is more simple than having to deal with labral repair. It just requires one to look beyond the hip joint and to fix the resting position of the femoral head. You SHOULD be able to cross your legs. If you can’t, start on the path to restoring that motion.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








