Muscle Minute TUESDAY – Adductor Magnus
Jack of All Trades – Meet the Adductor Magnus
Try this: Make a fist and using your knuckles and some pressure, run your hand along your inner thigh starting at your knee. Does it hurt? Is one side more sore than the other? You may have found the cause of your back pain, knee pain or pelvic floor problems. Let’s take a closer look:
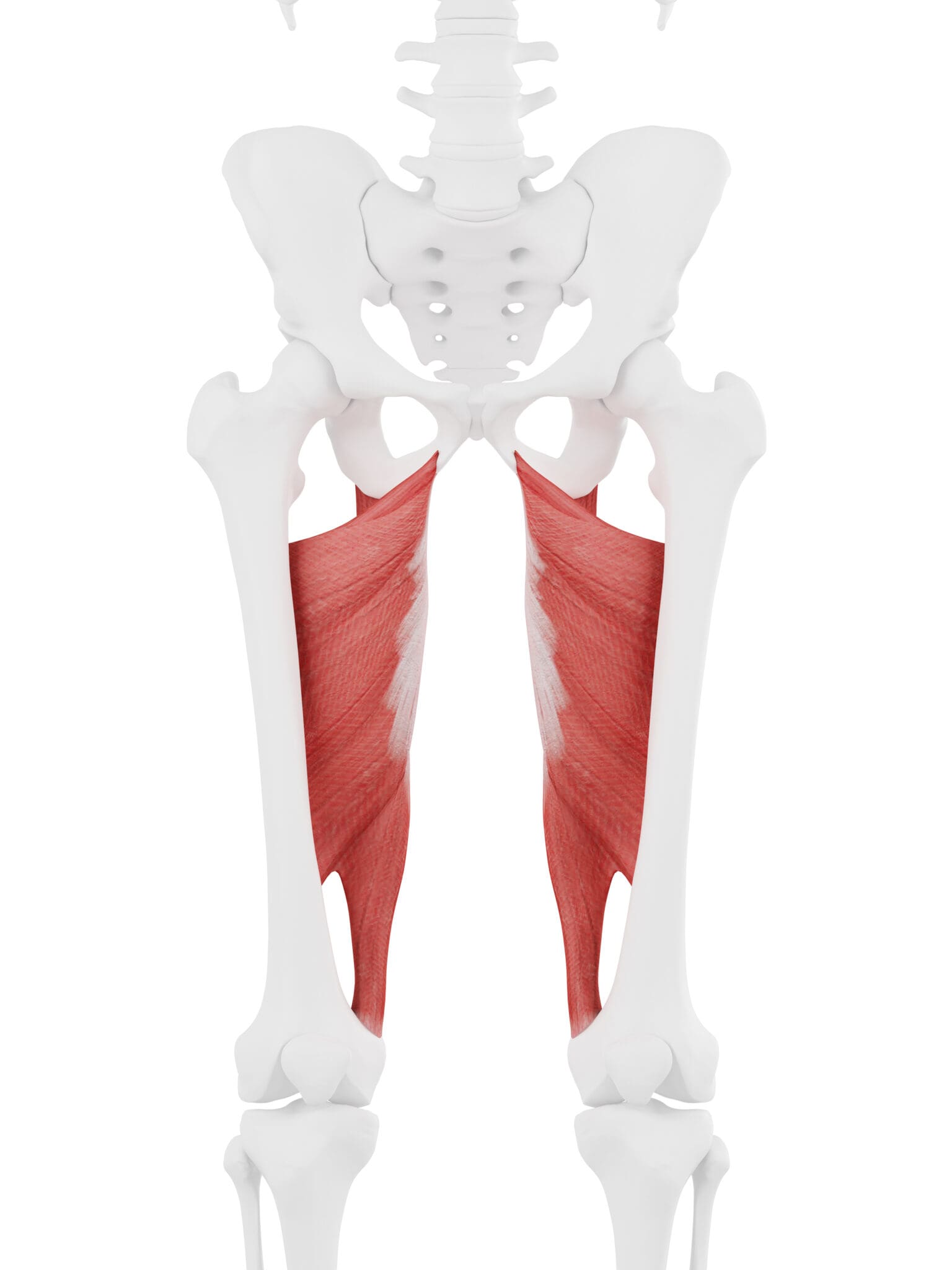
| Origin | pubis and ischial tuberosity |
| Insertion | linea aspera (femur) and adductor tubercle (femur) |
| Action | adduction, flexion (adductor portion), extension (hamstring portion) BUT when the foot hits the ground: deceleration of flexion (heel strike), abduction (mid stance) and concentric acceleration of hip ER (toe off) |
| Innervation | obturator n. (L2, L3, L4) sciatic n. (L4-S2) |
| Antagonists | gluteus medius |
The Real World Adductor Magnus
I became really intrigued by this muscle because I was finding severe fascial restrictions along the tendon near the adductor tubercle just above the knee and sometimes in the mid muscle belly of a lot of my patients. Notice how this muscle has an adductor portion AND a hamstring portion.
The hamstring portion originates from the ischial tuberosity and attaches at the midpoint of the femur where it joins in a fascial connection to the short head of the bicep femoris. It is why this muscle is sometimes called the 4th hamstring. When the foot hits the ground, this portion decelerates hip flexion to a higher degree than the gluteus maximus. That’s right, due to its large moment arm, the adductor magnus is a better decelerator of hip flexion than the gluteus maximus when the hip is flexed.
Where the hamstrings have a fascial connection from the ischial tuberosity through the sacrotuberous ligament to the lumbar extensors, the fascial connection of the adductor magnus is into the pelvic floor and the psoas major.
When patients ave had fascial restrictions in the adductor, that means the hip is chronically:
- adducted (person is over pronated, strengthen the gluteus medius)
- extended (person does not hinge well at the hip, teach the hip to flex)
- OR externally rotated (person is over supinated, strengthen the gluteus maximus in the transverse plane and teach them to walk with their toes pointed straight ahead and their big toe on the ground)
Here’s why this matters:
- Tight adductors may limit hip internal rotation, thereby limiting activation of the gluteus maximus
- If the adductor is strained, it may be because the gluteus maximus is weak. They are both external rotators of the hip as well as decelerators of hip flexion.
- Fascial tightness of the adductor may lead to pelvic floor insufficiency
- If the adductors are tight, the gluteus medius may be weak
Conventional thinking says: If the adductors are strained, strengthen them and stretch them. If they are tight, stretch them.
Real World Thinking says: If the adductor is strained, strengthen the gluteus maximus and if the adductor is tight (more common), release them with manual therapy and then strengthen the gluteus medius. If you have a patient with urinary stress incontinence, check this muscle for restrictions (pelvic floor connection) and if someone has low back pain, make sure to check this too (psoas connection).
Phew! If you made it to the end, you deserve a mental break. A long time ago, one of my staff members looked at me with an expression of exhaustion and said, “This was way easier when we did it the old [conventional] way.” Yeah, I know. But I promise this makes your day way more fun.
Because nobody has time to be in pain.
Until next time…