
Kinesiology THURSDAY – Psoas Major and Testicular Pain (Why did that work)
Here’s a case I treated a while back that has taught me a lot:
A firefighter presented with complaints of constant pain in the right lumbar area
radiating into the testicular region and B posterior thigh numbness. He states 12-13 years ago, a ceiling fell on him while he was fighting a fire. Two weeks later, his back “went out”. 2 years ago he began experiencing testicular pain and two weeks ago a discogram at L5 increased/reproduced his symptoms that are still lingering. He notices significant decrease in force with urination and was diagnosed with pudendal nerve irritation. He notes pain is almost always constant. He has had 9 lumbar injections (only one successful in decreasing pain two years ago in which he had total relief for 2 weeks).
Evaluation findings:
- Normal lumbar ROM except extension which was 25% and elicited LBP
- Severe left rotated pelvis
- Severe right psoas trigger point
- Pain with active right hip external rotation and abduction
- Associated trigger points noted in the right vastus lateralis, adductor magnus and medial hamstring
What fixed it?
Releasing the right psoas trigger point and surrounding fascia. Manually, this was accomplished with soft tissue mobilization, myofascial release and correction of pelvic alignment. Exercises were prescribed to encourage functional hip internal rotation. Why? The vastus lateralis and adductor magnus are external rotators of the hip and the medial hamstring is an internal rotator of the tibia.
Remember, trigger points set up in muscles that are chronically short. And the trigger point pattern and presence of left pelvic rotation were signs that the right hip was chronically externally rotated. Hip external rotation may present as someone toeing-out (over pronation) or someone rolling to the outside of their foot (over supination)
Exercises were also prescribed to activate the rectus femoris (a synergist to psoas major) and the abdominal muscles (antagonists to psoas major). Stretching the psoas is often considered a good intervention, but if the lumbar spine is already “extended” on that side due to psoas major hypertonicity, then the associated lumbar extension with hip flexor stretching may cause increased pain.
Why did that work?!
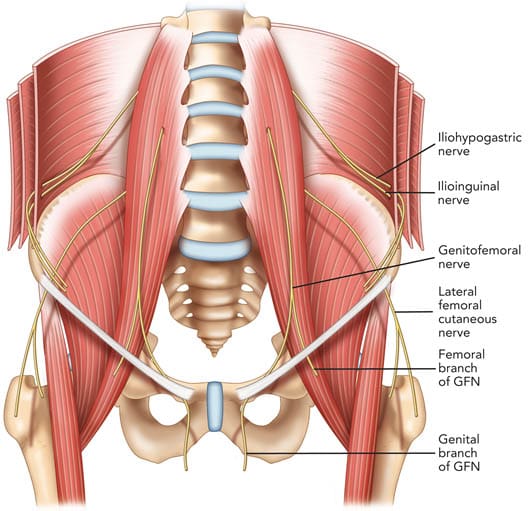
The genitofemoral nerve (L1, L2) pierces the psoas major and excessive and prolonged tightness of psoas major may impinge the nerve causing referred pain into the genital region. The psoas major originates from the transverse processes of L1-4 and the vertebral bodies of T12-L5, potentially causing lumbar nerve root compression and contralateral rotation of the lumbar segments if chronically tight. The psoas major is also a postural muscle prone to prolonged tightness if a femur is chronically externally rotated.
So next time you hear about lower back pain radiating into the genital region, think about the psoas major.
Because nobody has time to be in pain…for 12 years.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








