
Kinesiology THURSDAY – Patellar Tendonitis (Jumpers Knee)

Patellar tendinopathy (PT) plagues athletes of all ages, especially taking part in soccer, long-distance running, volleyball, basketball and ice hockey. According to a prospective study, more than 50% of the athletes with PT were forced to retire from active sport. Where many research studies focus on training surfaces, training intensity and gender difference, I thought I would take a moment to look at the kinesiological factors that may predispose someone to this overuse injury.
Here’s 5 things that make you go hmm…about jumping and tendon injuries:
- Tendons are often torn during eccentric loads
- Jumping creates ground reaction forces of 3-5x your body weight and with rates of force up to 500x your bodyweight per second
- A majority of the force occurs upon landing with the knee in 0˚-25˚ of flexion
- Repetetive microtrauma has been shown to be the cause of tendinopathy
Ever wonder why this injury often shows up only on one leg? People usually jump or land with both legs, right? So why does this problem primarily show up unilaterally? It’s worth it to take a second to look at the patellar tendon and see what makes it long and weak.
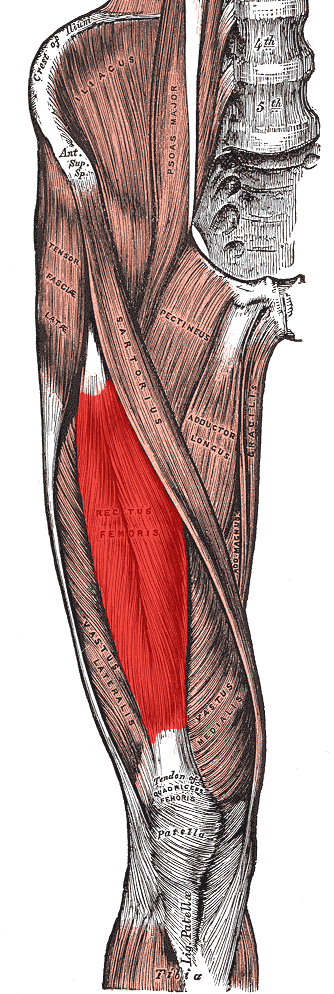
I purposely kept that whole picture in, so you would scroll down and observe the slightly inward path of the rectus femoris as it connects to the patella via the quadriceps tendon and then to the tibial tuberosity via the patellar tendon. Notice how that whole complex follows the gentle valgus angle of the knee. If I stare at this long enough, I can come up with a list of things that would place the patellar tendon in a long/weak position:
- Excessive knee valgus (frontal plane over pronation)
- Excessive tibial external rotation (or a femur that internally rotates too much)
- A trigger point in the rectus femoris (often associated with an anteriorly rotated innominate)
I know that was a heavy short list, but understanding the why behind the what can lead you to some excellent solutions that will combat this injury. Successful movement-based solutions include: (Check out our solution)
- Strengthening gluteus medius
- Strengthening gluteus maximus with the knee in 0˚-25˚ flexion
- Stretching the hamstrings in standing positions
And if you want to try some manual therapy, look out for:
- Trigger points in the gastrocnemius that may limit dorsiflexion (causing increased knee valgus)
- Trigger points in the adductor which will neurologically weaken the antagonist, the gluteus medius
- An anteriorly rotated innominate which makes a leg feel functionally longer (and long legs over pronate)
- Trigger points in the rectus femoris (which can cause #3 and also place increased tension on the distal patellar tendon)
Conventional thinking says: This is an overuse injury because the quad is weak and you need to rest and strengthen the quad.
Real World Thinking says: This tendon is placed on a weakened or neurologically inhibited position in someone that over pronates. The most common causes of over pronation:
- lack of ankle dorsiflexion
- weak gluteus medius (which then results in a weak gluteus maximus)
- an opposite limb that over supinates
I could go on about this for a few more hours. But it’s Thursday and we have to get to work. I know this kind of thinking can make your brain hurt, but your patients will thank you for it. Maybe one day we can discuss it live if you help me book a future seminar or if this problem is plaguing you, I would love to see if I can help you out. Or you can always meet me tomorrow for dessert first. Keep at it.
Because nobody has time to be in pain.
Until next time…
Kind Regards,
MoveWell Academy
[email protected]








